- Dengue virus is transmitted through the bites of infected Aedes mosquitoes. There are four serotypes of the virus.
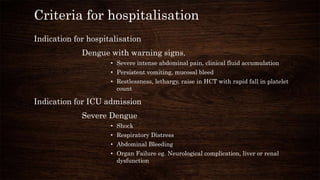
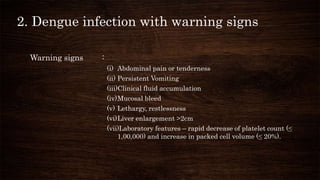
- Patients can be asymptomatic or experience symptoms ranging from undifferentiated fever to severe dengue with warning signs like abdominal pain or bleeding.
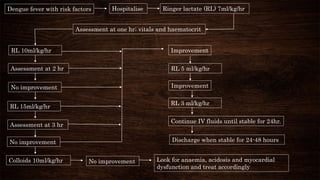
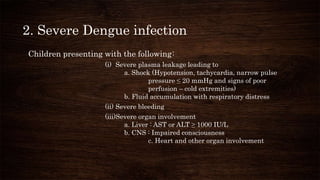
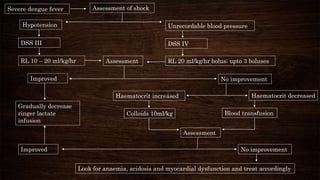
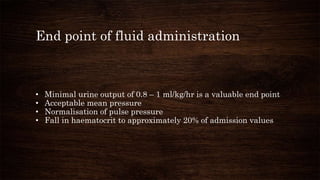
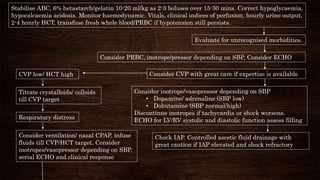
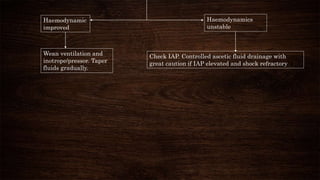
- Treatment depends on severity but involves rehydration and monitoring for warning signs. Hospitalization is needed for severe cases, and intensive care for life-threatening bleeding, shock, or organ involvement.