Downloaded 14 times



![5
Withdrawal [Cook 2001]
• Withholding or withdrawing….can be
orchestrated to occur quickly or slowly,
changing the tempo of the dying process
• PACE and SEQUENCE based on:
• 1. Potential suffering of patient
• 2. Vicarious suffering by others
• 3. Speed of death
EPILAT STUDY – France 2015](https://image.slidesharecdn.com/decisionmakingintheicuintensivecareunitbydr-170303122201/75/Decision-making-in-the-ICU-intensive-care-unit-by-Dr-Patrick-Neligan-Presentation-at-HFH-2016-conference-5-2048.jpg)






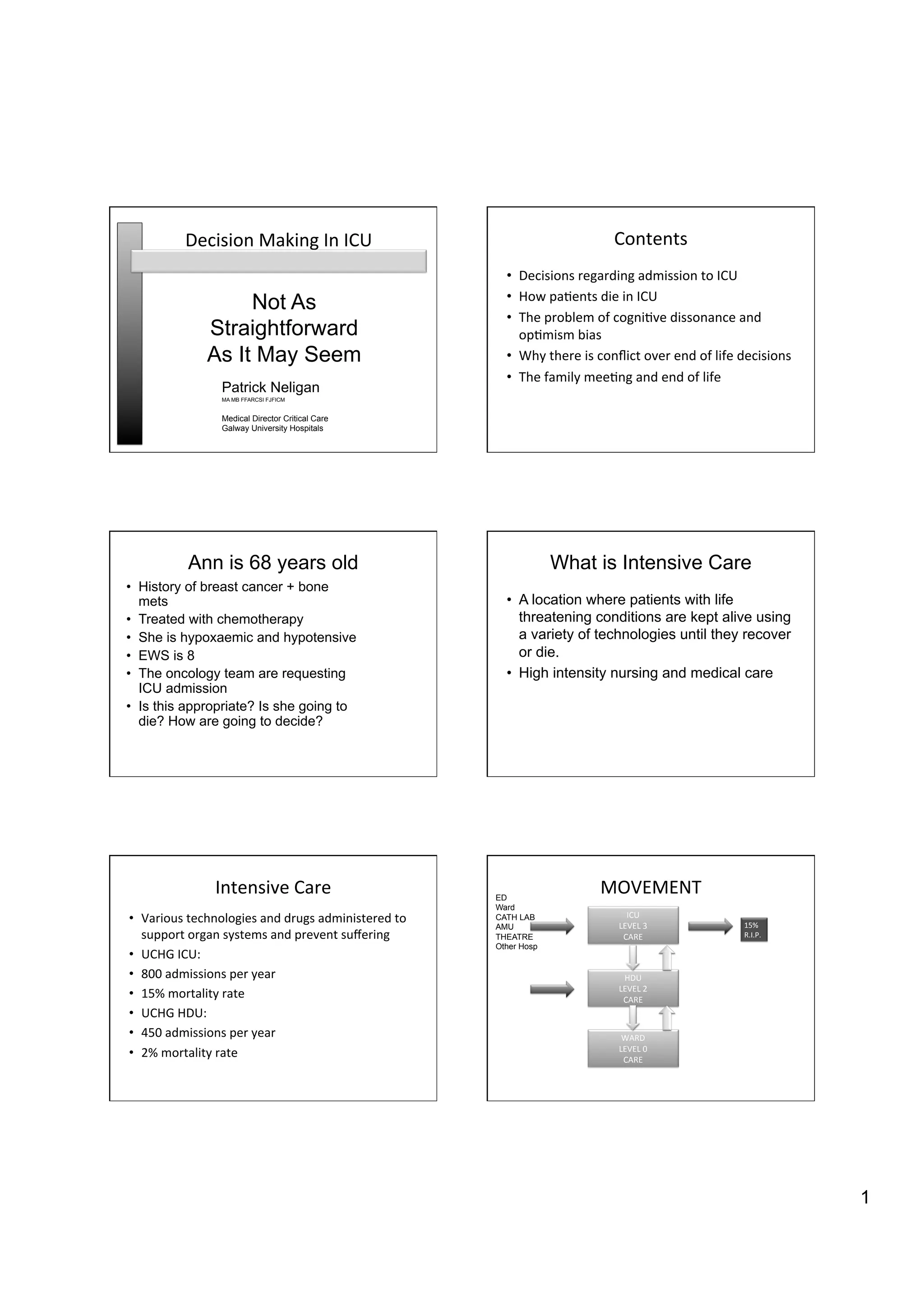
The document discusses decision-making in ICU regarding end-of-life care, focusing on critical issues such as patient admission criteria, cognitive biases, and communication strategies with families. It highlights the ethical implications of withholding or withdrawing life-support treatments and underscores the importance of structured family meetings to improve care and understanding. Key statistics include a 15% mortality rate among ICU patients, often within seven days of admission, primarily due to the withdrawal of life support.





































![Acute Hospital Network Agenda June 2015 [AHN 36]](https://cdn.slidesharecdn.com/ss_thumbnails/hfh-network-170320100219-thumbnail.jpg?width=640&height=640&fit=bounds)





![Acute Hospital Network Agenda June 2014 [AHN 24]](https://cdn.slidesharecdn.com/ss_thumbnails/hfh-network-agenda-17-june-2014ahn25june2014-170320100032-thumbnail.jpg?width=640&height=640&fit=bounds)




















![Presentation on DNAR Policy (From Acute Hospital Network, June 2014) [AHN 19]](https://cdn.slidesharecdn.com/ss_thumbnails/presentation-on-dnar-policy-dublin-june-2014ahn20june2014-170320094739-thumbnail.jpg?width=640&height=640&fit=bounds)










































