Downloaded 14 times

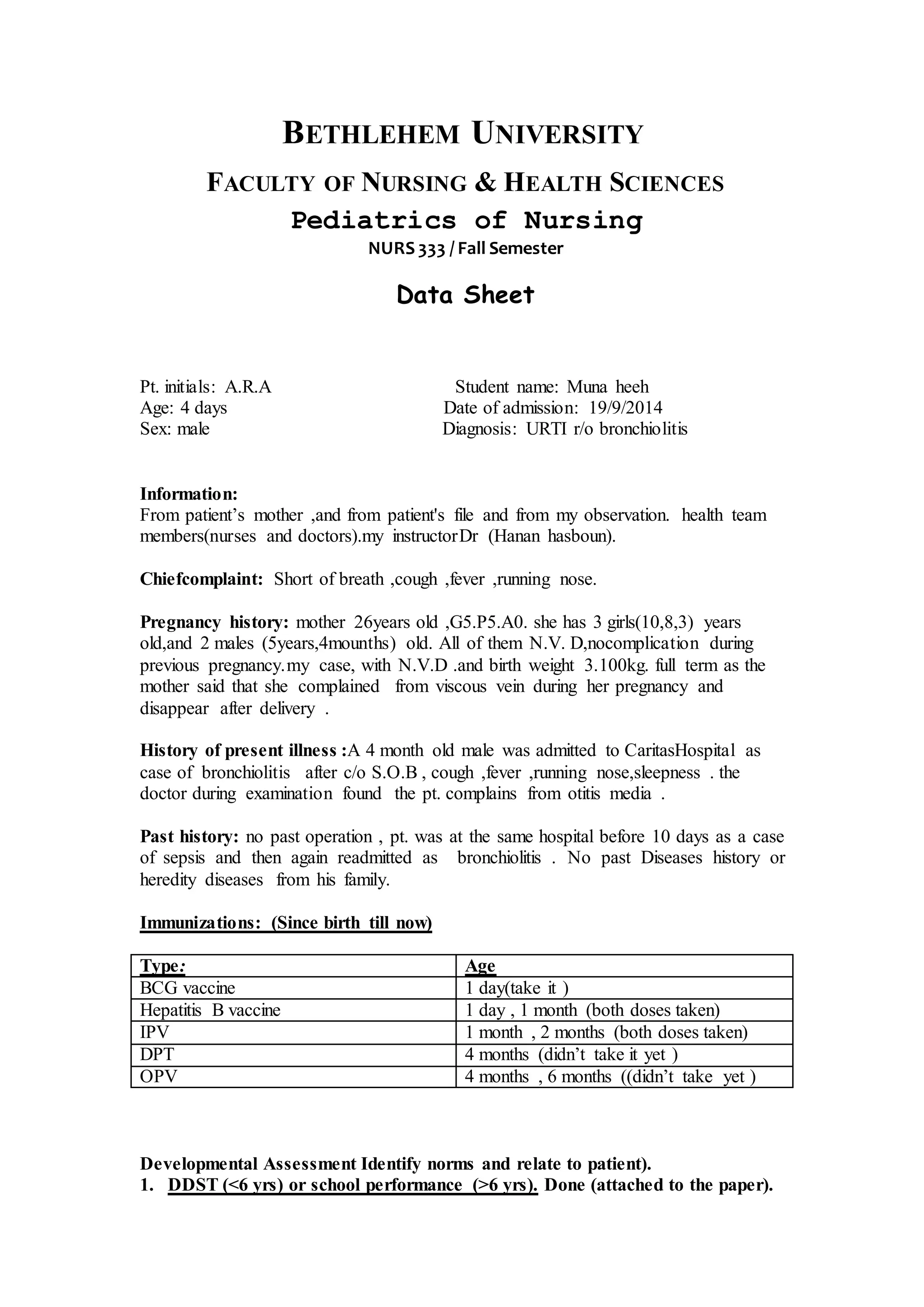

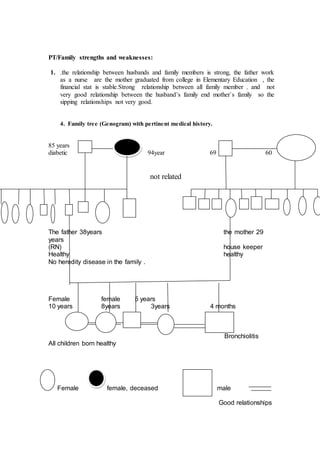



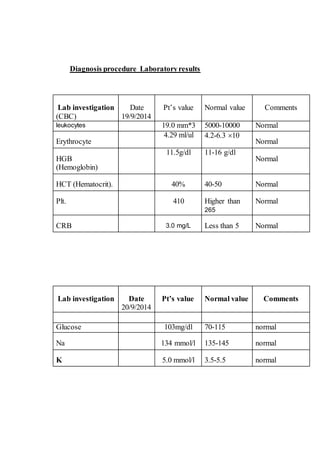

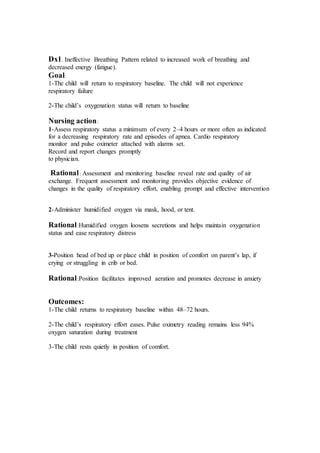







This document provides medical information about a 4-day-old male patient admitted to the hospital for bronchiolitis. It includes the patient's medical history, physical assessment, lab results, treatment including antibiotics and acetaminophen, and nursing care plan. The patient presented with shortness of breath, cough, fever and runny nose. Lab results were normal. He is being treated with ampicillin and acetaminophen and is improving with supportive nursing care including respiratory monitoring and oxygen administration.

































![congenital hypothyroid-1 - Copy [Autosaved].ppt](https://cdn.slidesharecdn.com/ss_thumbnails/congenitalhypothyroid-1-copyautosaved-250914060223-3616caf3-thumbnail.jpg?width=640&height=640&fit=bounds)

















![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)















