
Recommended
More Related Content
What's hot
What's hot (20)
Similar to Pregnancy skin changes
Similar to Pregnancy skin changes (20)
More from chandraushavns
Recently uploaded
Recently uploaded (20)
Pregnancy skin changes
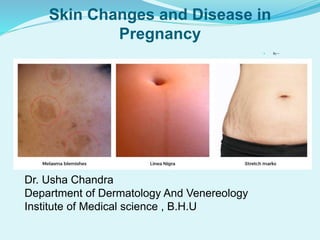
- 1. Skin Changes and Disease in Pregnancy By— Dr. Usha Chandra Department of Dermatology And Venereology Institute of Medical science , B.H.U
- 2. •Cutaneous changes results from the altered endocrine, metabolic and immunological milieus that characterize pregnancy •Cause physiological and pathological changes both
- 3. Pigmentery changes(most common) most marked in darker skin type due to oetrogen,progesterone ,MSH and other uncertain factors. 1.Generalized or increase in pigment at specific areas such as genital axillae, areolae, recent scars ,linea nigra.
- 4. 3.Melasma(chlosma , mask of pregnancy)-(70%) • Irregular,blotchy,symmetrical facial hyper pigmentation due to epidermal melanin deposition. • Due to combination of light exposure and elevated hormone( estrogen, progesterone and melanocyte stimulating hormone) • May regress postpartum.
- 5. 4.Darkening of ephelids and melanocytic nevi- Can be confused with malignant melanoma(age presentation). Can caused increase in dermoscopic Stole ABCD scoring system(Asymmetry, Border change ,Color, Diameter) & vascularity. Chan et al identified characteristic histological feature unique to nevi including increase in mitotic index.
- 6. Hair changes • During pregnancy, hair growth is more pronounced. • In second half of pregnancy, changes are due to androgen Hypertrichosis Hirsutism accompanied by acne(rarely virilization) • In postpartum, compensatory decrease in hair growth associate with shedding known as, telogen effluvium, which recover within 6 to 12 months. Mild frontoparietal recession may occur. Postpartum androgenic alopecia
- 7. Hair changes Androgenic alopecia Telogen effluvium
- 8. Nail changes – Subungual hyperkeratosis. Distil onycholysis. Transverse grooving. Brittleness of nail. Accelerated growth of nail. Longitudinal melanonychia
- 9. Vascular changes Occurs due to sustain high level of oestrogen. Changes are similar to those seen in hyperthyroidism or cirrhosis. 1. Spider angioma (spider nevi aranei)- These have central “ body” and small vessel (legs) extending out from it. Occurs on chest,leg,face. Disappear postpartum.
- 10. Vascular changes 2. Palmer erythema. 3. Non pitting edema(50%) of hands,ankles,face,feets more pronounced in early morning. 4. Varicosities of haemorrhoids ,leg(rare but serious complication of deep vein thombosis,occasionaly death occur d/t pulmonary embolism) 5. Cutis marmorata. 6. Hemangioendotheliomas, Unilateral neviods telangiectasia (unilateral dermatomal superficial telangiectasia)
- 11. Vascular changes 7. Vasomotor instability. 8. Dermatographism/ pruritis. 9. Pyogenic granuloma or granuloma gravidarum, pregnancy epulis. (5%) 10. Purpura 11. Gingival hyperemia or hyperplasia(2%)
- 12. Vascular changes Pyogenic granuloma Varicosities
- 13. Glandular function changes 1. Increased eccrine function (except palm) – It includes miliaria ,dyshydrotic eczema, hyperhydrosis 2. Increase sebaceous function- Growth in Montgomery’s tubercles, Acne (variant- pruritic folliculitis of pregnancy) It return normal after delivery. 3. Decreased apocrine function( improved Fox Fordyce disease). 4. Elevated thyroid activity with resultant relative iodine deficiency.
- 14. Structural changes during pregnancy 1. Striae distensae/gravidarum- Develop in 90% of pregnant in second third trimester. Pink to purple atrophic band at right angle of skin tension Most common over abdomen, breast, thigh, buttock. 2. Molluscum fibrosum gravidarum
- 15. Mucosal changes 1. Jacquemier – Chadwick sign – It is bluish discoloration of vagina and cervix 2. Goodell’s sign – cervical softening. 3. Gingivitis (marginal gingivitis, papillomatous hypertrophy of gums )
- 16. SKIN INFECTIONS AFFECTING PREGNANCY Human papilloma virus (condyloma lata) Herpes simplex Varicella zooster HIV infection Scabies
- 17. HUMAN PAPILLOMA VIRUS Also k/a Condyloma acuminata. Exacerbated or grow rapidly in second trimester. Contain of epidermal or dermal papule or nodule on perineum genital or crural fold or anus, of varying size.(Occasionally obstructing birth canal) Physical treatment should be done(cryotherepy,electrocautery) Prevention – bivalent vaccine (Cervarix) against 16 & 18 and quadrivalent (Gardasil) against 6,11,16,18.
- 19. HUMAN PAPILLOMA VIRUS Infant have high risk of laryngeal papillomatosis (HPV 6 and 11) No link has been found between HPV and miscarriage, premature delivery, or other pregnancy complications.
- 20. HERPES SIMPLEX VIRUS Primary herpetic infection occur in 2% of pregnancy More severe than non pregnant. HSV1 is associated with herpetic gingivostomatitis and pharyngitis. Reactivation involves outer one third of lower lips, most common. HSV-2 involve genitalia (10 to 40% by HSV-1)
- 21. Development of vesicles, ulcer or hard crusts starting with erythema and papule and then followed by dry flaking and residual swelling. Primary and recurrent genital infection is indication of caesarean section and treatment (acyclovir). Babies with low birth weight infection can be life theatening HSV can be vertically transmitted to the infant before, during, or after delivery, although intrapartum transmission accounts for most cases.
- 22. HERPES SIMPLEX VIRUS Herpes Labialis Genital herpes
- 23. Varicella zoster Primary VZV infections occur in upto 1:2000 pregnancy. Primary infection have risk of pneumonia and encephalitis (both in mother and child) ,spontaneous abortion, fetal demise, and varicella embryopathy (eg, limb hypoplasia, microcephaly, muscle atrophy, cataracts, and mental retardation). Reactivation of latent varicella is not associated with faetal risk High risk of fetal varicella syndrome (1-2%) infection during 13 to 20 weeks of gestation. Treatment should be done with intravenous or oral acyclovir.
- 24. Varicella zooster Multiple, discrete, vesiculopustular, and maculopapular lesions on an erythematous base Neonatal infection may occur in 10% to 20% of neonates whose mothers became acutely infected from 5 days before delivery to 2 days after the delivery.
- 25. Scabies Caused by the human mite Sarcoptes scabiei var hominis Areas affected include the fingers webs,flexor surfaces of the wrist, axillae, waist, feet and ankles Primary lesions are the first manifestation of the typically include small papules, vesicles, and burrows(S shaped). Secondary lesions are the result of rubbing and scratching,they may be the only clinical manifestation.
- 26. Scabies No faetal risk. First line of treatment is topical permethrin 5%, and antihistamine to reduce ithching. oral ivermectin is not safe
- 27. HIV infection Skin disease which are characteristic of HIV are- Oral hairy leukoplakia ,Bacillary angiomatosis ,Kaposi sarcoma. • ART can be given during labor or pregnancy. • C section is considered if viral load is high. • Breast feeding should be avoided. • HIV positive infant should given pneumocystic prophylaxis with co trimoxazole.
- 28. Oral Hairy - Bacillary angiomatosis Kaposi sarcoma leukoplakia
- 29. Auto immune disorder in pregnancy Systemic lupus erythematosus Pemphigus vulgaris and foliaceus.
- 30. Systemic lupus erythrematosis Immune system in pregnancy cause shift from predominantly TH1 lymphocyte to TH2 profile. Level of IL-12 and gamma interferon are reduced and level of IL-4 10 are increased. So increase in susceptibility to skin disease like SLE. About 60% of women with pre existing SLE have flare during pregnancy or puerperium.
- 31. Systemic lupus erythrematosis Cutaneous flare are most common. Fetal risk includes– spontaneous abortion, faetal loss, preterm delivery, intra uterine growth restriction. Corticosteroids are drug of choice but not reduce flares. It can be associated with APLA syndrome with increased risk of thromboembolism.
- 32. PEMPHIGUS Pemphigus vulgaris and foliaceus can both develop and worsening during pregnancy. The primary lesion of pemphigus vulgaris is a flaccid blister filled with clear fluid that arises on healthy skin or on an erythematous base. Clinical symptom is similar to pemphigoid gestationalis. Featal prognosis is variable. Fetal skin shares same desmoglein3 profile as in oral adult mucosa.
- 33. PEMPHIGUS Flaccid bulla of pemphigus DIF of skin biopsy
- 34. PEMPHIGUS Treatment ladder- First line- prednisolone Second – azathioprine Third- plasma exchange,plasmapheresis
- 35. INFLAMMATORY SKIN DISEASE Pustular psoriasis of pregnancy( impetigo herpetiformis) Acne vulgaris and rosacea Pityriasis rosea Urticaria
- 36. Pustural psoriasis of pregnancy or Impetigo herpetiformis Psoriasis typically improve during pregnancy, but in 10 to 20 % it can worsen. It is variant of Pustural psoriasis due to hormonal alteration during pregnancy Classically during last trimester but occur as early as first trimester resolve after delivery. Typically on flexures, spreads centrifugally sometimes generalized. Mucosa rarely involves. Sparing face palm and soles.
- 37. Pustural psoriasis of pregnancy Characterized by acute eruption of erythematous patches whose margin are studded with sub corneal pustules with constitutional symptoms(eg. Fever, tetany,hypocalcemia)
- 38. Laboratory investigation shows anemia, leucocytosis neutrophilia, increase in ESR, hypoalbuminia. Histopathology shows typical changes of pustular psoriasis with parakeratosis and abscesses of neutrophils (Kogoj's spongiform pustules). Recurrence with subsequent pregnancy are common and characteristically more severe with onset earlier in gestation. Featal risk – Placental insufficiency, stillbirth or neonatal death. Pustural psoriasis of pregnancy
- 39. Pustural psoriasis of pregnancy Treatment ladder— First line- emollients, topical steroids(low to mild ) Second line- narrow band UV-B or Braod Band UV-B Third line-Ciclosporin ,systemic corticosteriod in impetigo herpetiformis(second and third trimester),tumor necrosis factors(adalimumab, etanercept, infliximmab)
- 40. Acne vulgaris Occurs due to blockage and/or inflammation of pilosebaceous units . Affecting face (mostly ),back and chest. Occurs due to increase in androgen level. It improve early but worsen in third trimester. Acne conglobata( severe) may require systemic corticosteroids with or without oral antobiotic. Acne neonatoram may occur due to passive transfer of materal androgen across placenta.
- 41. Acne vulgaris acne vulgaris acne conglobata
- 42. Acne Rosacea Due to increase level of oestrogen. Affects the central region of the face presenting itself as a flushing of the face, and then redness develops with small red bumps and cysts similar to acne vulgaris Rosacea fulminans is rare variant that may flare in pregnancy.
- 43. Acne vulgaris and acne rosacea Treatment ladder – First line- topical (azelic acid 10 -15%), benzoyl peroxide gel (2.5 – 10%), oral erythromycin (avoid in first trimester), oral azithroymycin. Second line- narrow band UV-B Third line- prednisolone( can be combine by oral antobiotic) Retinoid(oral / systemic) are avoided
- 44. Pityriasis Rosea Caused by HHV-6. Oval scaly plaque on trunk preceded by “herald patch”. Can be asscociated with fetal demise (in first trimester) premature delivary. Treatment is conservative as rash fades.
- 45. Urticaria Differential diagnosis include pre bullous phase of pemphigoid gestationis or polymorphic eruption of eruption Treatment – First line- topical emollient(aqueous cream and 1-2 % menthol), oral histamines(loratadine and cetrizine). Second line- prednisolone.
- 46. Itching in pregnancy Pruritus gravidarum Occurs in one – fifth. Intense pruritis in absence of primary cutaneous changes. Mostly due to some underlying cause(urticaria,eczema,etc) Mid form of reccurrent intra hepatic cholestasis of pregnancy
- 47. Intra hepatic cholestasis of pregnancy • Also known as obstetric cholestasis, cholestasis of pregnancy, recurrent(45 to 75%) jaundice of pregnancy, cholestatic jaundice of pregnancy, idiopathic jaundice of pregnancy, icterus gravidarum, prurigo gravidarum(ie.pruritis is not accompanied by jaundice). • It is reversible(resolve within 2 to 4 weeks of after pregnency). • Multifactorial cause (hormonal, genetic , environmental and alimentary factor) which induce biochemical changes in susceptible pregnancy.
- 48. Intra hepatic cholestasis of pregnancy Moderate to severe pruritis, begin during first (10%) and second (25%) trimester. Localized to palm and soles or generalized. Primary cutaneous lesion are invariably absent but intense pruritis associated with secondary excoriation. Progress to clinical jaundice(10%), often with constitutional symptoms after 1 to 4 weeks of pruritis. Second cause of jaundice in pregnancy followed by viral hepatitis.
- 49. Intra hepatic cholestasis of pregnancy Laboratory studies- Shows increase in serum bile acids(single sensitive indicator) and correlates with degree of pruritis Brites et al indentify following features- 1. Sr. TBA > 11 µM (normal 4.6 to 8.7 µM) 2. Cholic acid : chenodeoxycholic acid > 1.5 ( 0.7 to 1.5) or choric acid proportion of TBA greater than 42% 3. Glycine conjugate:taurine conjugate of bile acids <1.0(0.9 to 2.0) or glycocholic acid concentration greater than 2.0 (0.6 to 1.5 µM)
- 50. Intra hepatic cholestasis of pregnancy Histopathology of skin not aid in diagnosis. Liver biopsy reveals intrahepatic cholestasis with dilated , plugged bile canaliculi and deposites of bile pigment. Fetal risks – Increased rates of prematurity,intrapartal distress and fetal death,intra/postpartum haemorrhage. It generally correlated with acute placental anoxia and increased of meconium stained amniotic fluid. Treatment is ursodeoxychilic acid , enhance efficiency achieved by co administration with S- adenosylmethionine.
- 51. Intra hepatic cholestasis of pregnancy Treatment ladder- First line- topical emollient(aqueous cream and 1-2 % menthol), oral histamines(loratadine and cetrizine), oral UDCA 15mg/kg/day. Second line- S-adenosyl-L-methionine, dexamethasone, cholestyramine. Other- weekly CTG, maternal vitamin K replacement,dexamethasone for fetal lung maturity.
- 52. SPECIFIC DERMATOSIS Polymorphic eruption of pregnancy. Pemphigoid gestationalis Atopic eruption of pregnancy
- 53. Pruritic urticarial papules and plaques of pregnancy (Polymorphic eruption of pregnancy) • Also known as Bourne’s toxemic rash of pregnancy, nurse late onset PP, toxic erythema of pregnancy • Occurs in 1 in 160 pregnancies ,self limiting, primigravida, in last trimester or immediate post partum (15%), may recur in next multiple pregnancy. • Aetiology- Abdominal distension leads to damage to connective tissue due to overstreching. Hormonal or imunological plays minimal role
- 54. Pruritic urticarial papules and plaques of pregnancy Lesions are polymorphous,(most commonly, urticarial) of 1 to 2 mm surrounded by narrow pale hollow, typically begin within striae on abdomen and thigh, papule may coalesce to form plaque , vesicle may present (never bulla) sparing periumblical region ,face , palm and sole.
- 55. Pruritic urticarial papules and plaques of pregnancy Laboratory investigations are normal, decreased serum cortisol. Histopathology shows nonspecifically, parakeratosis, spongiosis with dermal edema and lymphocytic, eosinophilic, neutrophilic infiltrate. DIF is negative. Duration of symptoms averaging 6 weeks of duration with spontaneous remmission is the rule. no adverse fetal outcome.
- 56. Pruritic urticarial papules and plaques of pregnancy • Treatment ladder- First line- topical emollient(aqueous cream and 1-2 % menthol), oral histamines(loratadine and cetrizine), toical steroids, Second line- Prednisolone consider early induction of labour if patient is close to term
- 57. Pemphigoid (herpes) gestationis • Auto immune, pruritic ,rare roughly 1 in 50,000 pregnancies. • It presents during late pregnancy (2nd or 3rd trimster, mean onset 21st week) or immediate post partum. • A mismatch HLA antigens between the mother and father, manifested by immunologic response against the paternal class II antigens( BP-180 or bullous pemphigoid antigen 2) at placental BMZ with cross reaction at the skin BMZ.
- 58. Pemphigoid (herpes) gestationis •Acute onset, intensely pruritic urticarial lesions on abdomen(typical site) in 50% of cases with rapid progression to generalized ,pemphigoid like eruption. Sparing -- face,mucous membrane, palm and sole
- 59. Pemphigoid (herpes) gestationis • The rash wax and wanes during pregnancy ,only to flare during labor and delivery(75%) or post partum(25%). Can associated with trophoblastic tumours (choriocarcinoma, hydatid moles) and Increased risk of other auto immune disease like Grave’s disease. Foetal risk– A. Newborn affected upto 10% of the time typically mild and self limiting. B. Slight increase in premature and small for gestational age birth(not affected by treatment taken i.e. Corticosteroids)
- 60. • •Lab. investigations are normal(serum complements) •Histopathology shows sub epidermal vesicles with perivascular infiltrate of variable no. of eosinophils(more common) and lymphocytes. • DIF( Gold standard) shows C3(100%) with or without IgG in a linear band along basement membrane zone • PG ELISA test may replace IF though not all patient react with BP120 (NC16A site)
- 61. Pemphigoid (herpes) gestationis Treatment ladder- First line- topical emollient(aqueous cream and 1-2 % menthol), oral histamines(loratadine and cetrizine), potent topical steroids, Second line- Prednisolone(0.5 -1 mg/kg/day) Third line- azathioprine, plasma exchange, i.v. Ig
- 62. Atopic eruption of pregnancy It is diagnosis of exclusion. Most common dermatosis(50%) ,75% cases occur before third trimester. Associated with reccurrence with good prognosis. A. E type or eczematous type- (two third) also known as eczema of pregnancy in second or third trimester consist of eczematous patches and plaques flexural extremity,face neck chest are involved.
- 63. Atopic eruption of pregnancy B. P type or papular type - (one third) Also known as prurigo of pregnancy, Besnier’s prurigo gestationalis, nurse’s early onset prurigo of pregnancy, papular dermatitis of Spangler, atopic eruption of pregnancy Excoriating or crusted erythematous papules present. Lesion present on extremities,occasionally on trunk, shin and arms. Key features is severe dryness, atopic minor feature according to Hanifin & Rajka.
- 64. Atopic eruption of pregnancy Treatment ladder- First line- topical emollient,oral histamines(loratadine and cetrizine), topical steroids, Second line- Narrow Band UV B Third line- Azathioprine, Prednisolone
- 65. THANK YOU
Editor's Notes
- Neonatal infection may occur in 10% to 20% of neonates whose mothers became acutely infected from 5 days before delivery to 2 days after the delivery.
- Acne conglobata (AC) is an uncommon and unusually severe form of acne characterized by burrowing and interconnecting abscesses and irregular scars (both keloidal and atrophic), often producing pronounced disfigurement. The comedones often occur in a group of 2 or 3, and cysts contain foul-smelling seropurulent material that returns after drainage. The nodules are usually found on the chest, the shoulders, the back, the buttocks, the upper arms, the thighs, and the face.[1]Acne conglobata may develop as a result of a sudden deterioration of existing active papular or pustular acne, or it may occur as the recrudescence of acne that has been quiescent for many years. See the images below.
- Rf includes numerous pustule marked facial erythema, cystic swelling coaelese sinus.