2. Introductio
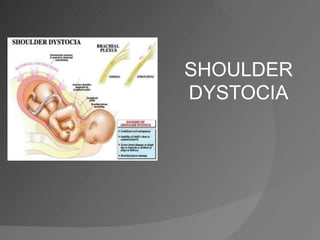
nz Shoulder dystocia
Ø Delivery that requires additional obstetric maneuvers
to release the shoulders after gentle downward
traction has failed.
Ø Occurs when the fetal anterior shoulder or less
commonly, posterior shoulder impacts against the
maternal symphysis or sacral promontory following
delivery of the vertex
Ø An obstetric emergency and one of the most
frightening event in labour room.
Ø Unpredictable and unpreventable event.
3. z Calm and effective management of this emergency is
possible with recognition of the impaction and institution
of specified maneuvers.
z Incidence : 0.2% to 3.0% of all vaginal deliveries
z Conventional risk factors predicted only 16% of shoulder
dystocia that resulted in infant morbidity hence risk
assessments for the prediction of shoulder dystocia are
insufficiently predictive to allow prevention of the large
majority of cases.
z Clinicians should be aware of existing risk factors but
must always be alert to the possibility of shoulder dystocia
with any delivery.
4. Risk factors and
anticipation
Only 25% of shoulder dystocias have at least 1 risk factorq Maternal
v
v
v
Abnormal pelvic anatomy
Short stature mother
Gestational diabetes mellitus
v Post-dates pregnancy
v Previous history of shoulder dystocia
v Maternal BMI >30
q Fetal
v Suspected macrosomia (>4500g)
q Labor related
v Assisted vaginal delivery (forceps or vacuum)
v IOL
v Prolonged active phase of first-stage labor
v Prolonged second-stage labor
v Secondary arrest
v Augmentation of labor
5. Ø Most of the prenatal and antenatal risk factors for shoulder
dystocia are interrelated with FETAL MACROSOMIA.
Ø However large majority of infants with a birth weight of
≥4500g do not develop shoulder dystocia and 48% of
incidences of shoulder dystocia occur in infants with a birth
weight <4000g.
Ø Clinical fetal weight estimation is unreliable and
third-trimester ultrasound scans
have at least a 10% margin for
error for actual birth weight and
a sensitivity of just 60% for
macrosomia (over 4.5 kg).
6. Case-control study
ž Objective : To determine if shoulder dystocia can be predicted in
babies born weighing 3.5kg or more.
ž A case–control study nested in a perinatal database of 899
mothers and their babies who weighed 3.5kg or more. All were
term pregnancies and delivered vaginally. A case was defined
as any baby that encountered shoulder dystocia at delivery.
Controls were deliveries over the same period that were not
complicated by shoulder dystocia. A logistic regression model
was created with macrosomia, parity, previous delivery of more
than 3.5kg, diabetes in pregnancy, prolonged labor, prolonged
second stage and instrumental delivery as the independent
variables. The adjusted odds ratio and the receiver operator
characteristics (ROC) curves were used to see if these
variables, both individually and as a model, were associated
with or were discriminative enough to predict shoulder dystocia;
an ROC curve of more than 0.7 showing good prediction.
Asmah Mansor, Kulenthran Arumugam, Siti Zawiah Omar
Department of Obstetrics & Gynaecology, University of Malaya Medical Centre,
(Eur J Obstet Gynecol Reprod Biol. 2010 Mar;149(1):44-6. Epub 2009 Dec 29.)
7. ž Result : There were 36 cases of shoulder dystocia during
the study period, an incidence of 4%. Previous delivery of
more than 3.5kg, prolonged labor and prolonged second
stage were not associated with shoulder dystocia.
Although diabetes and instrumental delivery were
independently and significantly associated with shoulder
dystocia their importance as a predictor became relevant
only in the presence of macrosomia.
ž Conclusion : Macrosomia is the only reliable predictor of
shoulder dystocia in babies weighing 3.5kg or more
Asmah Mansor, Kulenthran Arumugam, Siti Zawiah Omar
Department of Obstetrics & Gynaecology, University of Malaya Medical Centre,
(Eur J Obstet Gynecol Reprod Biol. 2010 Mar;149(1):44-6. Epub 2009 Dec 29.)
8. Preventio
nv Induction of labour
§ DM mother on insulin à reduce the risk of macrosomia and risk of
shoulder dystocia but does not reduce maternal or neonatal morbidity
§ Women without DM at term with suspected macrosomic baby à
no evidence to support that shoulder dystocia can be prevented with
IOL
v Caesarian section
§ Mother with DM + suspected big baby should be considered for
ELLSCS to
r
e
d
u
c
e
th
e
p
o
te
n
t
ia
l
m
o
r
b
id
ity
§ Not recommended in non-DM mother with suspected big baby
§ Mode of delivery for mother with previous history of shoulder dystocia
à for mother/obstetrician to decide.
§ N
o
r
e
q
u
i
r
e
m
e
n
t
t
o
a
d
v
i
s
e
E
L
L
S
C
S
r
o
u
t
in
e
ly
b
u
t
b
e
lo
w
f
a
c
t
o
r
s
s
h
o
u
ld
a
l
l
b
e
c
o
n
s
id
e
r
e
d
w
h
e
n
o
f
f
e
r
in
g
r
e
c
o
m
m
e
n
d
a
t
io
n
s
f
o
r
t
h
e
n
e
x
t
d
e
l
iv
e
r
y
:
1.
th
e
s
e
v
e
r
ity
o
f
a
n
y
p
r
e
v
io
u
s
n
e
o
n
a
ta
l
o
r
m
a
t
e
r
n
a
l
in
j
u
r
y
,
2.
fe
t
a
l
s
iz
e
3.
m
a
t
e
r
n
a
l
c
h
o
i
c
e
9. Diagnosing in
laborb
d
n
t
Difficulty with delivery of the face and
chin
The head remaining tightly applied to
the vulva or even retractingà ‘turtle
sign’
Failure of restitution of the fetal head
Failure of the shoulders to descend.
Royal College of Obstetricians and Gynaecologists Clinical Guideline-Guideline No 42
Shoulder Dystocia, December 2005
10. z Shoulder dystocia becomes obvious when the
fetal head emerges and then retracts against
the perineum, commonly referred to as the
“turtle sign.”
11. The CESDI (Confidential Inquiry Into Stillbirth and
Death in Infancy) report on shoulder dystocia
identified that 47% of the babies died within 5
minutes of the head being delivered.
Therefore it is important to manage the problem as
efficiently as possible but also carefully :
Ø Efficiently so as to avoid hypoxia acidosis
Ø Carefully so as to avoid unnecessary trauma
12. Intrapartum
managementØ M
O
/o
b
s
t
e
t
r
ic
ia
n
t
o
s
t
a
n
d
b
y
a
t
s
e
c
o
n
d
s
t
a
g
e
o
f
la
b
o
u
r
w
h
e
n
s
h
o
u
ld
e
r
d
y
s
t
o
c
ia
i
s
a
n
t
ic
ip
a
t
e
d
.
Ø H
o
w
e
v
e
r
,
i
t
i
s
r
e
c
o
g
n
iz
e
d
t
h
a
t
n
o
t
a
l
l
c
a
s
e
s
c
a
n
b
e
a
n
t
ic
ip
a
t
e
d
a
n
d
t
h
e
r
e
f
o
r
e
a
l
l
b
i
r
t
h
a
t
t
e
n
d
a
n
t
s
s
h
o
u
ld
b
e
r
e
a
d
y
w
i
t
h
th
e
te
c
h
n
iq
u
e
s
r
e
q
u
i
r
e
d
to
fa
c
i
l
i
t
a
t
e
d
e
l
iv
e
r
y
c
o
m
p
l
ic
a
t
e
d
b
y
s
h
o
u
ld
e
r
d
y
s
t
o
c
ia
.
15. z
z
Episiotomy is not necessary for all cases.
Some authors have advocated that episiotomy is an essential
part of the management in all cases. The authors of one study
have concluded that episiotomy does not decrease the risk of
brachial plexus injury with shoulder dystocia.
An episiotomy should therefore
be considered……….
but it is NOT MANDATORY!
Evaluate for
Episiotomy
16. Leg à The McRoberts
Maneuverž It
straightens
the
lumbosacral
angle,
rotates
the
maternal
pelvis
cephalad
and
is
associated
with
an
increase
in
uterine
pressure
and
amplitude
of
contrac8ons.
ž The
McRoberts’
maneuver
is
the
single
most
effec8ve
interven8on,
with
reported
success
rates
as
high
as
90%
with
low
rate
of
complica8on
Royal College of Obstetricians and Gynaecologists Clinical Guideline-Guideline No 42
Shoulder Dystocia, December 2005
17. Ø Fundal pressure should not be employed.
It is associated with an unacceptably high neonatal
complication rate and may result in uterine rupture.
Ø Maternal pushing should be discouraged, as this
may lead to further impaction of the shoulders,
thereby exacerbating the situation.
18. Suprapubic
Pressurea.k.a Rubin I
maneuverž
ž
ž
Apply
with
downward
and
lateral
direc8on
to
push
the
posterior
aspect
of
the
anterior
shoulder
towards
the
fetal
chest
for
30sec
(recommended
8me).
Either
con8nuous
pressure
or
‘rocking’
movement
Reduces
the
bisacromial
diameter
and
rotates
the
anterior
shoulder
into
the
oblique
pelvic
diameter.
Gobbo R, Baxley EG. Shoulder dystocia. In: ALSO: advanced life support in obstetrics provider course
syllabus. Leawood, Kan.: American Academy of Family Physicians, 2000.
20. Internal rotation
maneuvers
Mr. Kim Hinshaw, consultant obstetrician and gynecologist, Newcastle, England.
In: ALSO ®: advanced life support in obstetrics instructor course syllabus. Leawood,
Kan.: American Academy of Family Physicians, 2002:67.
21. ž
Removal of posterior
arm
Delivery of the posterior arm has a high complication
rate (12% humeral fractures) but the neonatal trauma
may be a reflection of the refractory nature of the
case, rather than the procedure itself.
22. Roll the patients to her hands and
knees (All Four Position)
ž 83% success rate in one case series
23. What measures should be taken
if first and second-line
maneuvers fail?
zThird-line maneuvers require careful consideration
to avoid unnecessary maternal morbidity and
mortality.
zIt is difficult to recommend a time limit for the
management of shoulder dystocia, as there are no
conclusive data available.
24. Last resort
maneuvers!!1. Cleidotomy
2. Symphysiotomy
3. Zavanelli maneuver
Royal College of Obstetricians and Gynaecologists Clinical Guideline-Guideline No 42
Shoulder Dystocia, December 2005
25. Symphysioto
myz Has been suggested as a potentially useful
procedure, both in the developing and developed
world.
z High incidence of serious maternal morbidity and
poor neonatal outcome.
z After delivery, the birth attendants should be alert
to the possibility of postpartum haemorrhage and
3rd/4th degree perineal tears.
26. Zavanelli
manoeuvrez Cephalic replacement of the head, and delivery
by Caesarean section has been described but
success rates vary.
z Zavanelli maneuver may be most appropriate for
rare bilateral shoulder dystocia
z The maternal safety of this procedure is unknown,
however should be borne in mind, knowing that a
high proportion of fetuses have irreversible
hypoxia-acidosis by this stage.
27.
28. Complicatio
nsz Maternal
ø Postpartum hemorrhage (11%)
ø Third- or fourth-degree episiotomy or tear
(3.8%)
ø Uterine rupture
ø Symphyseal separation or diathesis,
with or without transient femoral neuropathy
ø Rectovaginal fistula
z Fetal
ø Brachial plexus palsy (4-16%)
ø Clavicle fracture
ø Fracture of the humerus
ø Fetal hypoxia, with or without permanent
neurological damage
ø Fetal death
29. Erb-Duchenne Palsy (80%)
(C5-C6)
Klumpke’s Palsy
(C7-T1)
• Moro reflex is absent
• Grasp of the hand is present.
• Fingers and wrist have normal motion.
• Impaired functions of deltoid, the external
rotators of the shoulder, elbow flexors and
wrist extensors (supraspinatus, infraspinatus
and teres minor, biceps brachii, brachialis,
supinator, and the brachioradialis).
• Shoulder is adducted and internally rotated.
• The elbow is extended and the forearm
pronated (the “waiter’s tip position”)
•
•
•
•
•
Moro reflex present/absent,
Loss of grasp reflex.
Wrist flexors, long digital flexors, and the
intrinsic muscles of the hand are impaired,
Muscles controlling the shoulder and elbow
are usually spared.
The hand is supinated, the wrist extended,
and the fingers clawed
31. z
z
z
z
z
Brachial plexus injuries are one of the most important fetal
complications of shoulder dystocia, complicating 4–16% of
such deliveries.
Most cases resolve without permanent disability, with fewer
than 10% resulting in permanent brachial plexus
dysfunction.
Neonatal brachial plexus injury is the single most common
cause for litigation related to shoulder dystocia.
Not all injuries are due to excess traction by the
accoucheur and there is now a significant body of evidence
that maternal propulsive force may contribute to some of
these injuries
Evidence from cadaver studies suggests that lateral and
downward traction is more likely to cause nerve avulsion
Brachial plexus
injuries
32. Documentation
z It is important to record :
● time of delivery of the head
● direction the head is facing after restitution
● maneuvers performed, their timing and sequence
● time of delivery of the body
● staff in attendance and the time they arrived
● condition of the baby (Apgar score)
● umbilical cord blood acid-base measurements.
Royal College of Obstetricians and Gynaecologists Clinical Guideline-Guideline No 42
Shoulder Dystocia, December 2005