Download to read offline
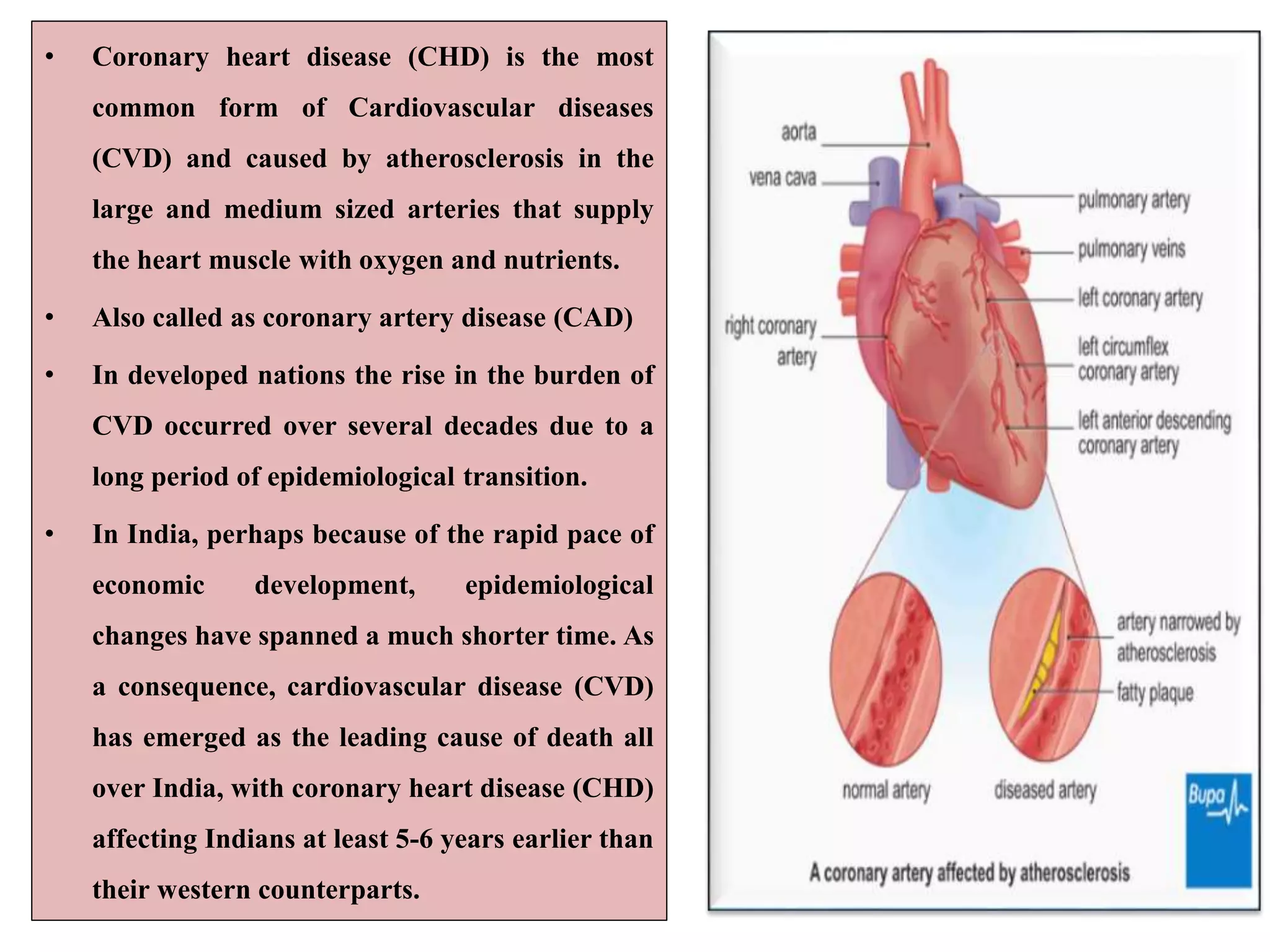
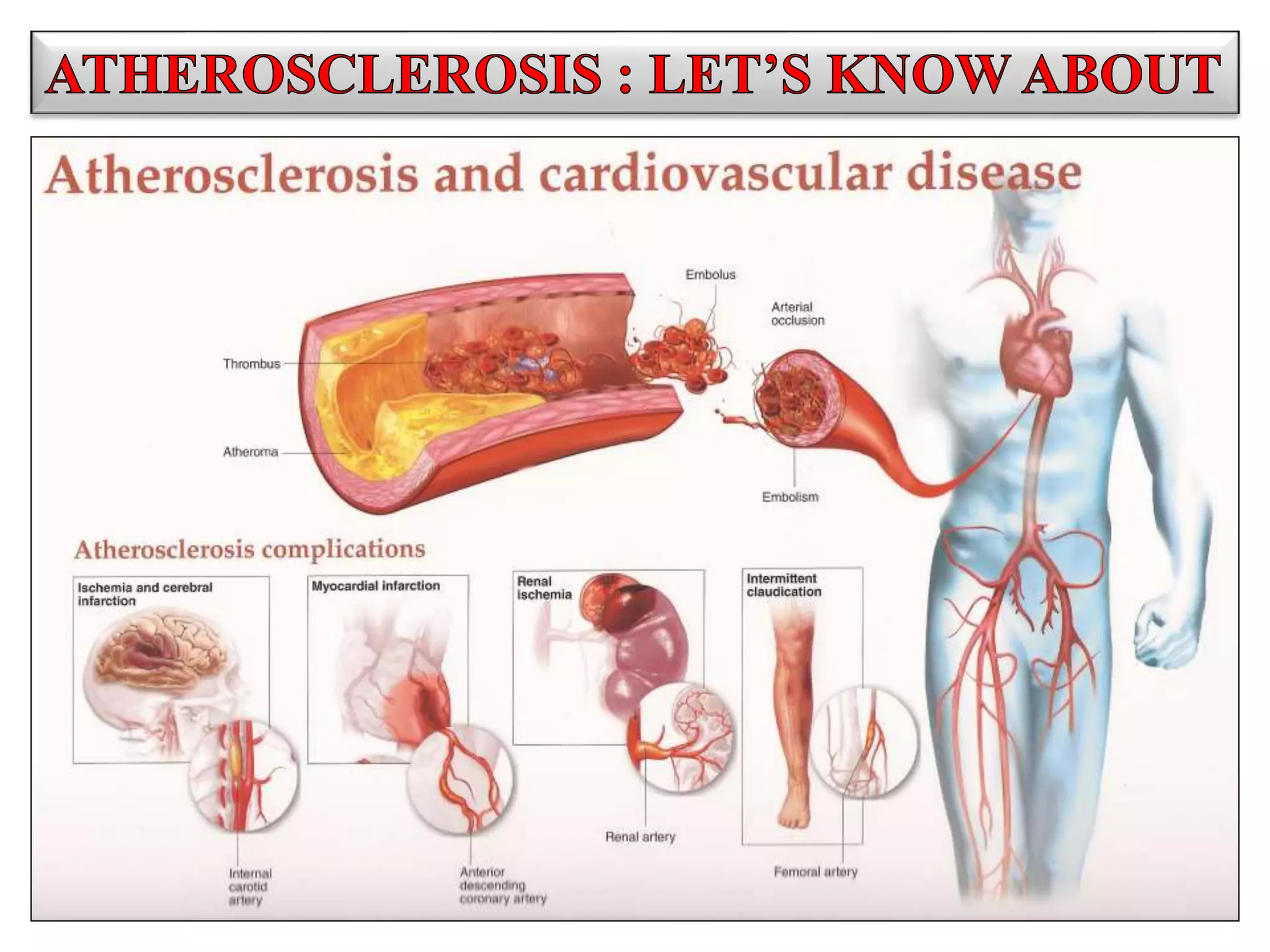
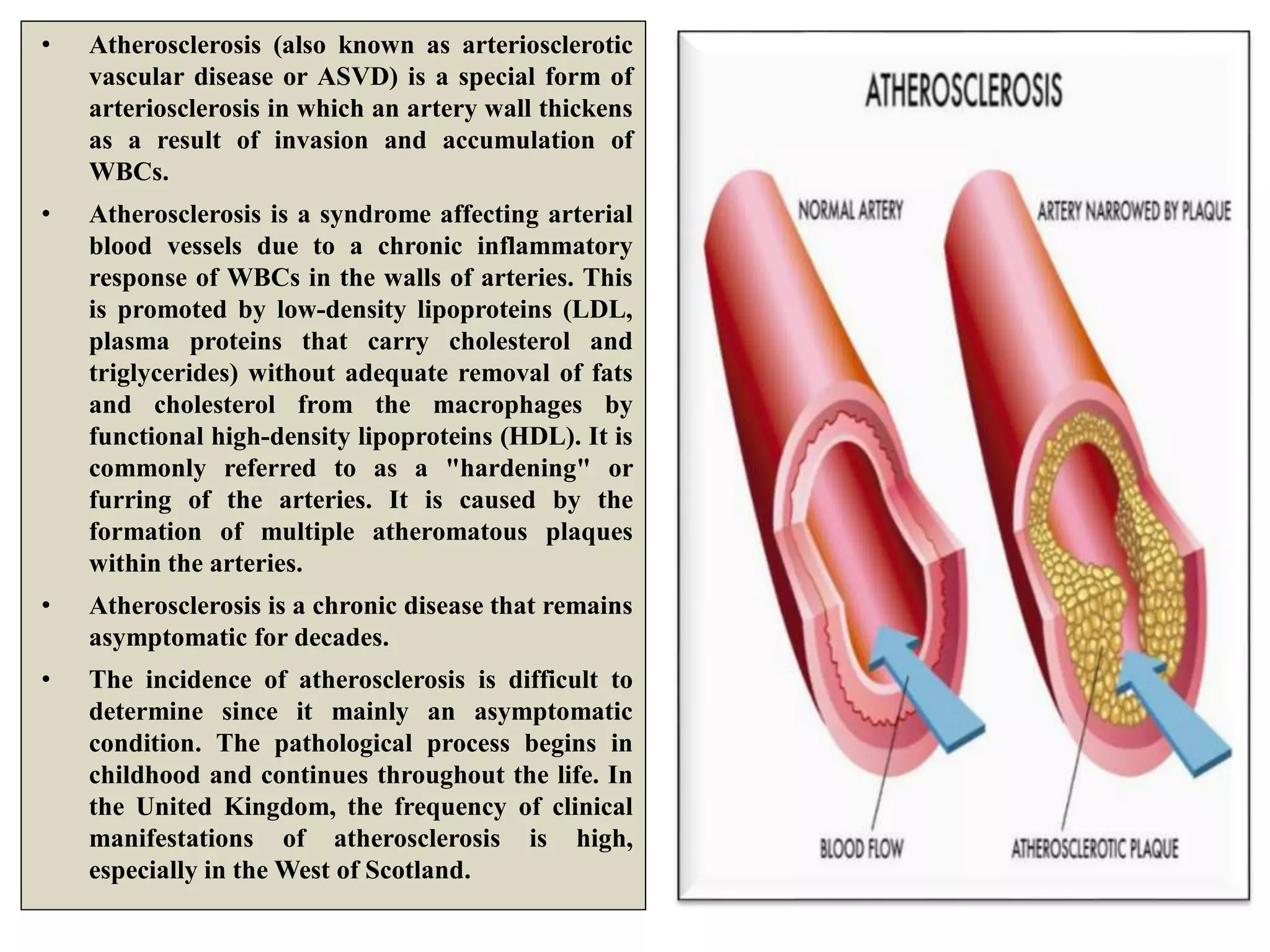
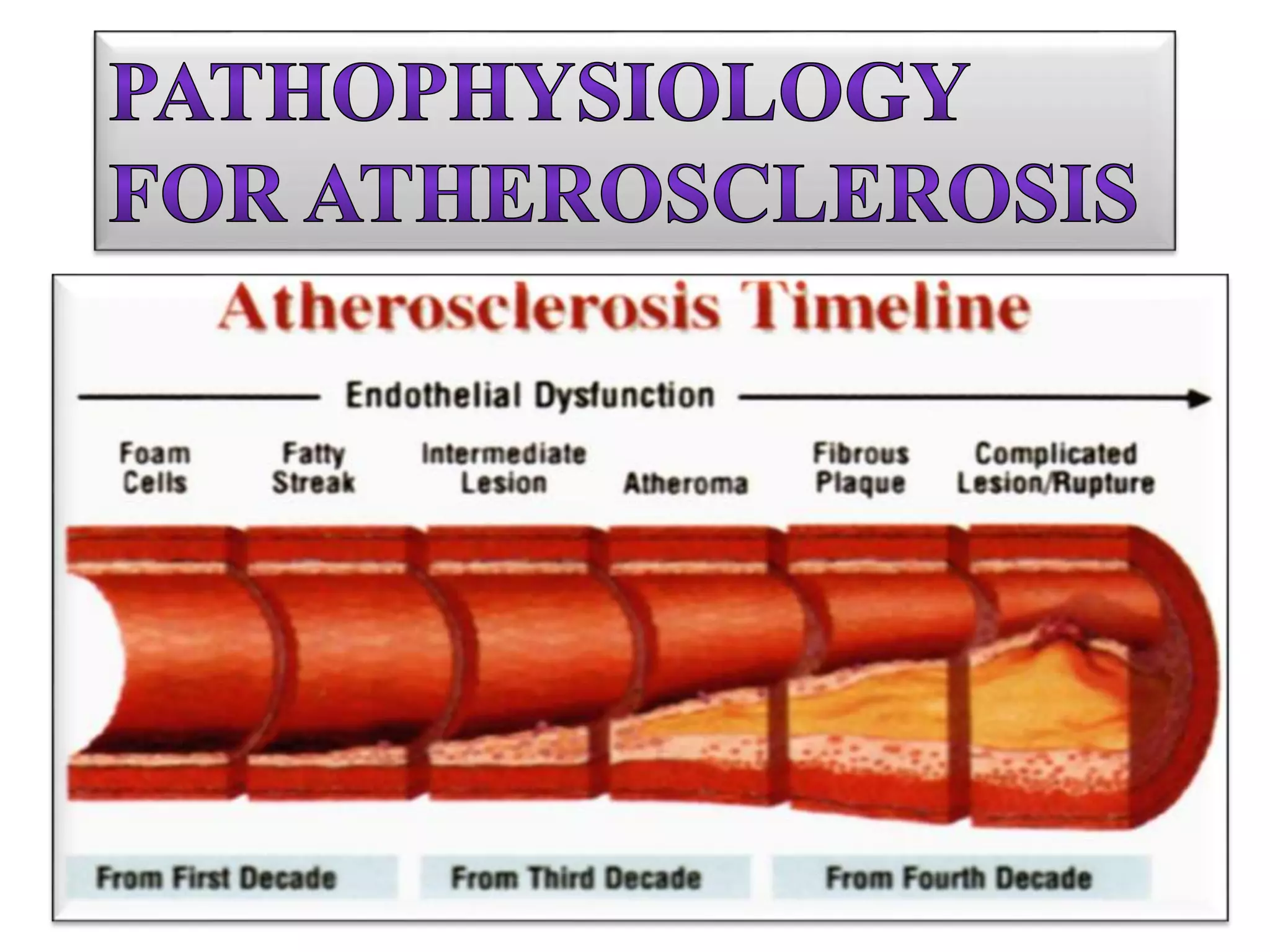
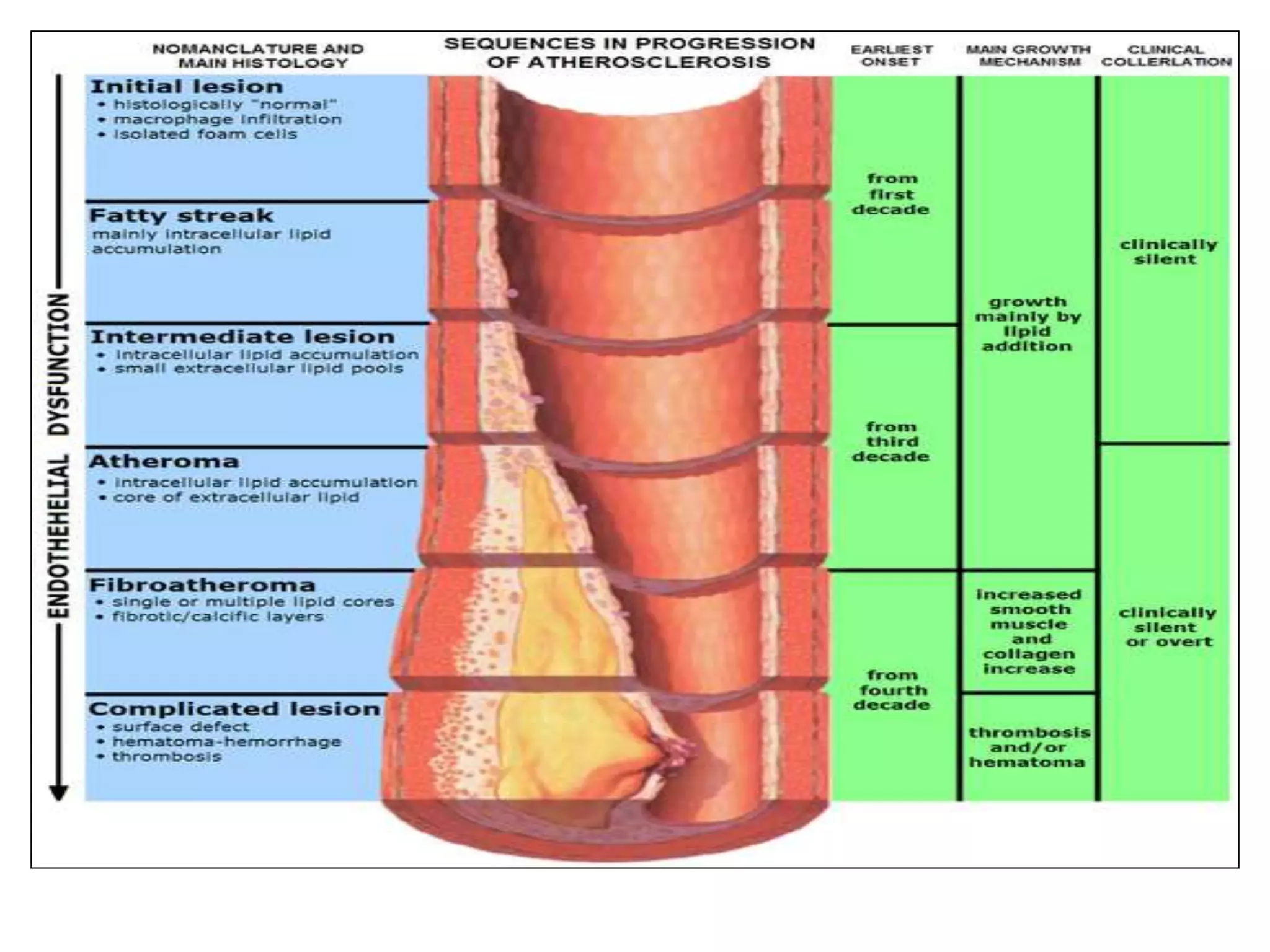
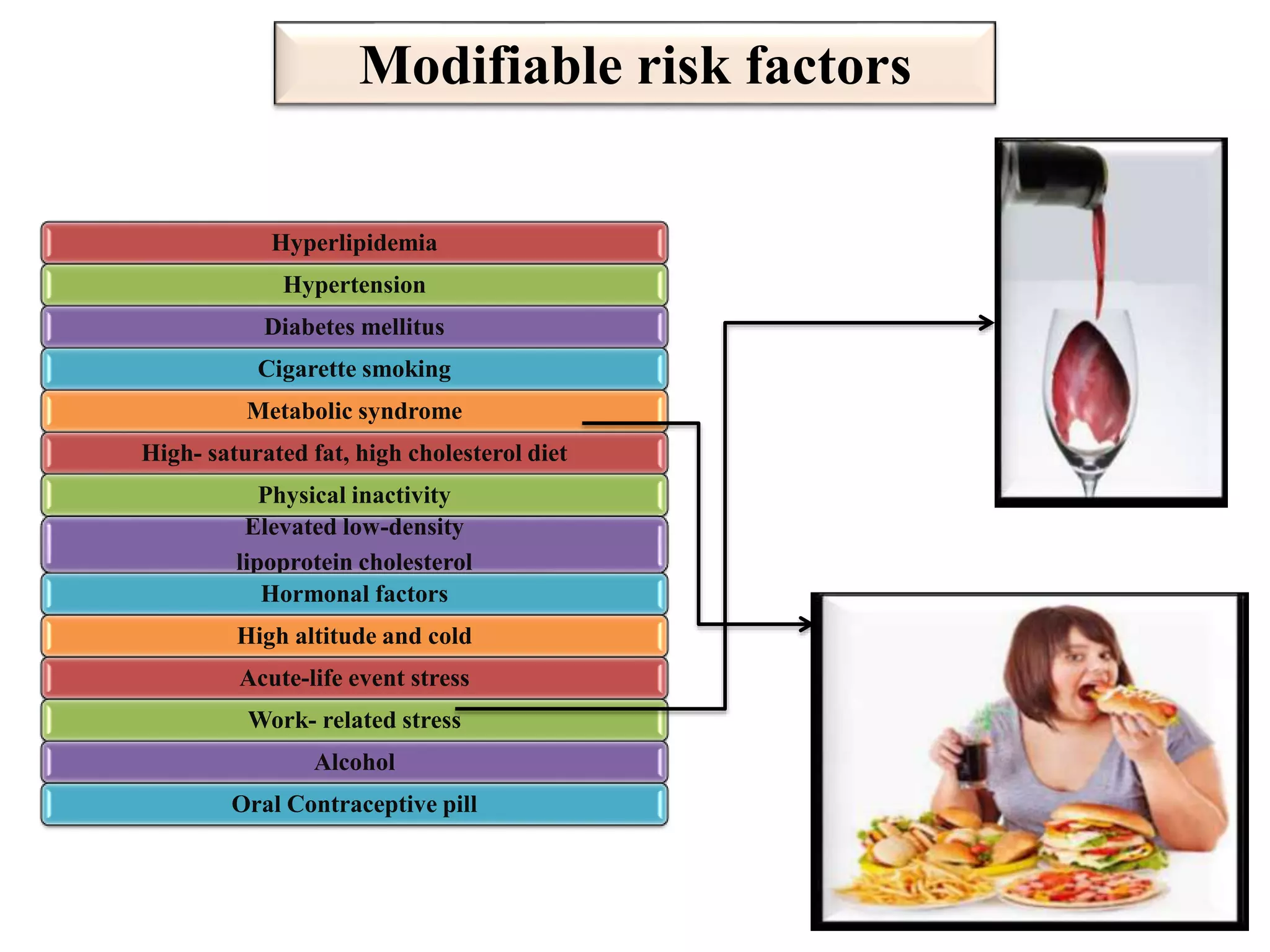
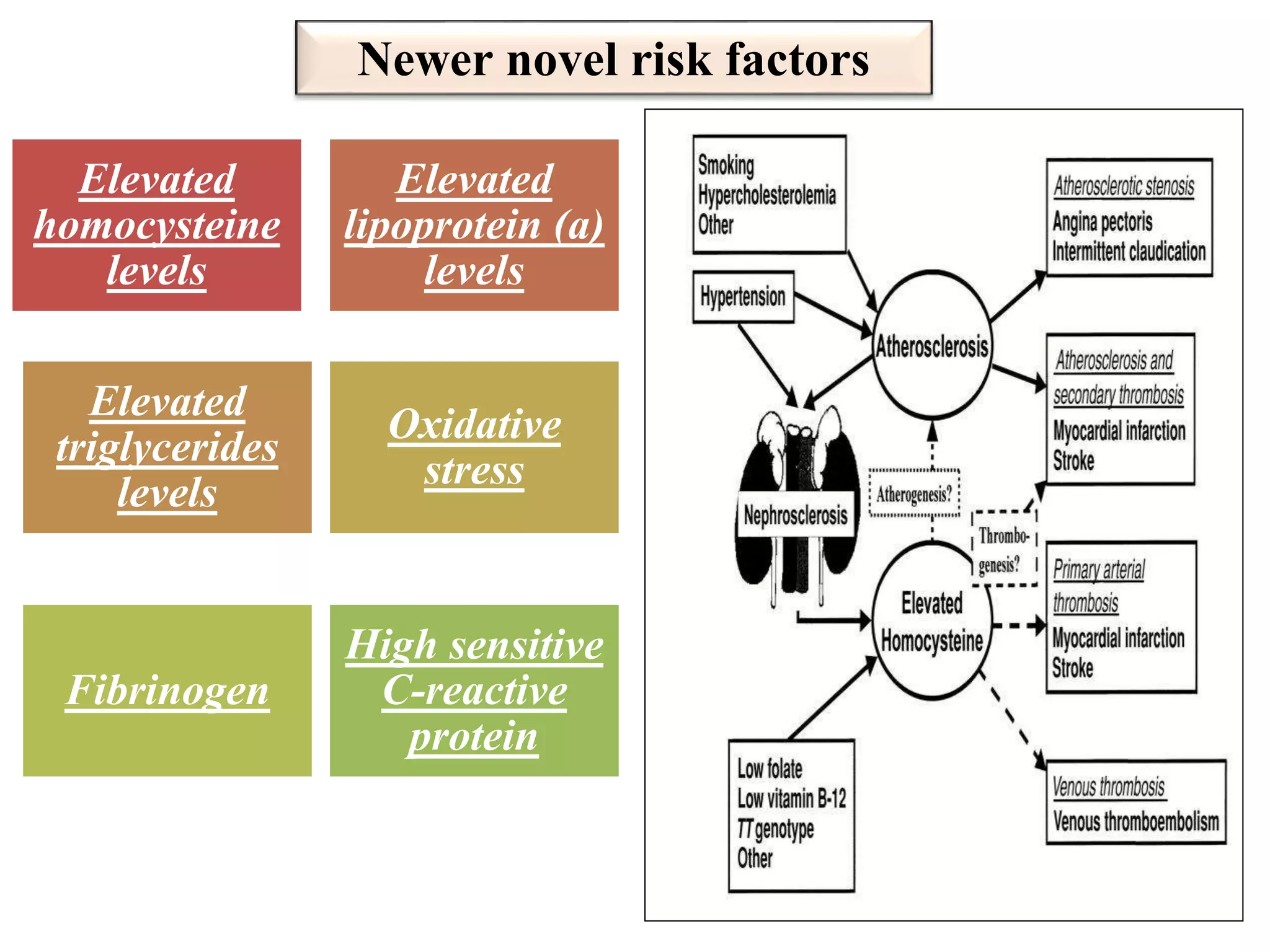
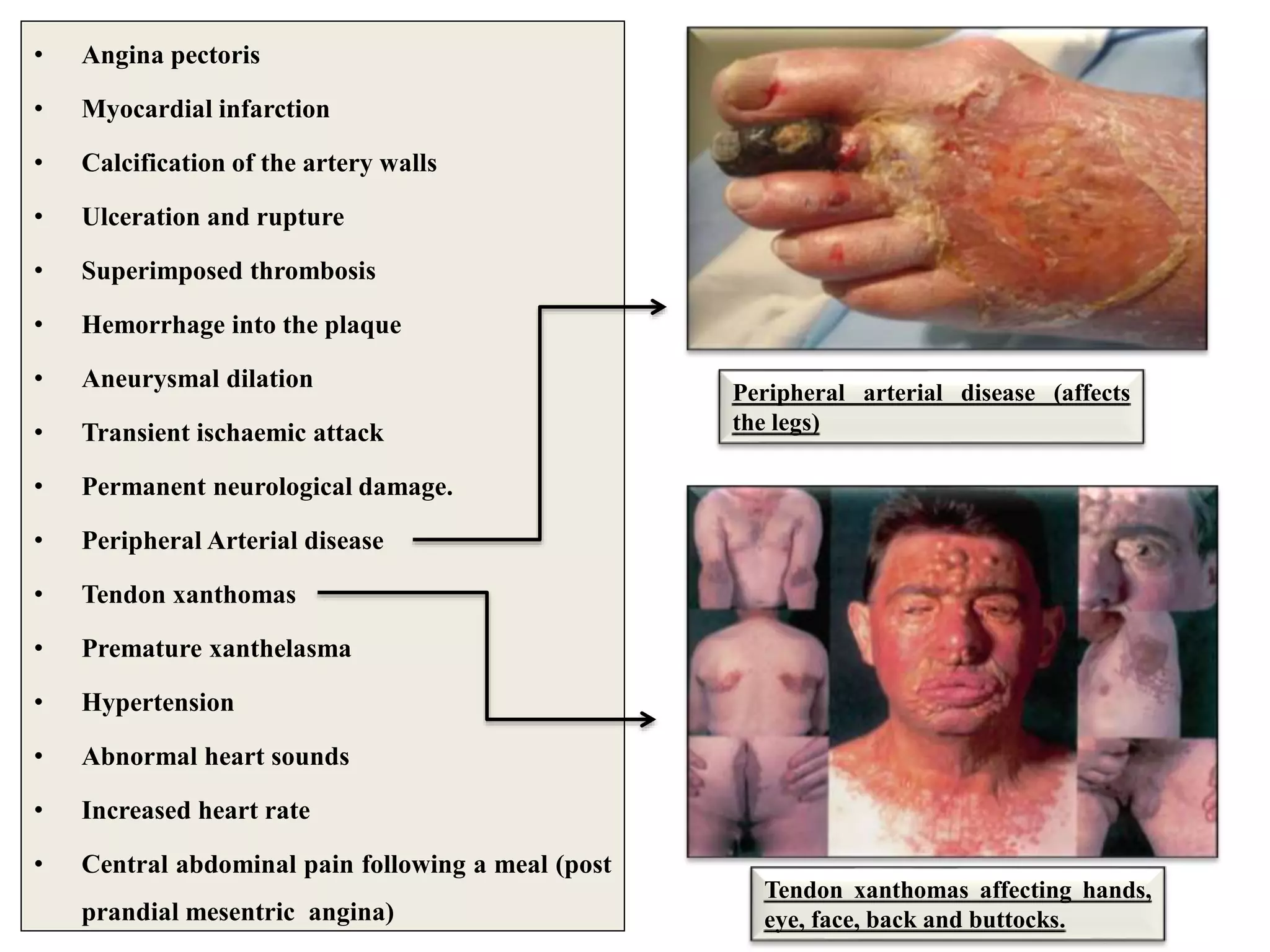





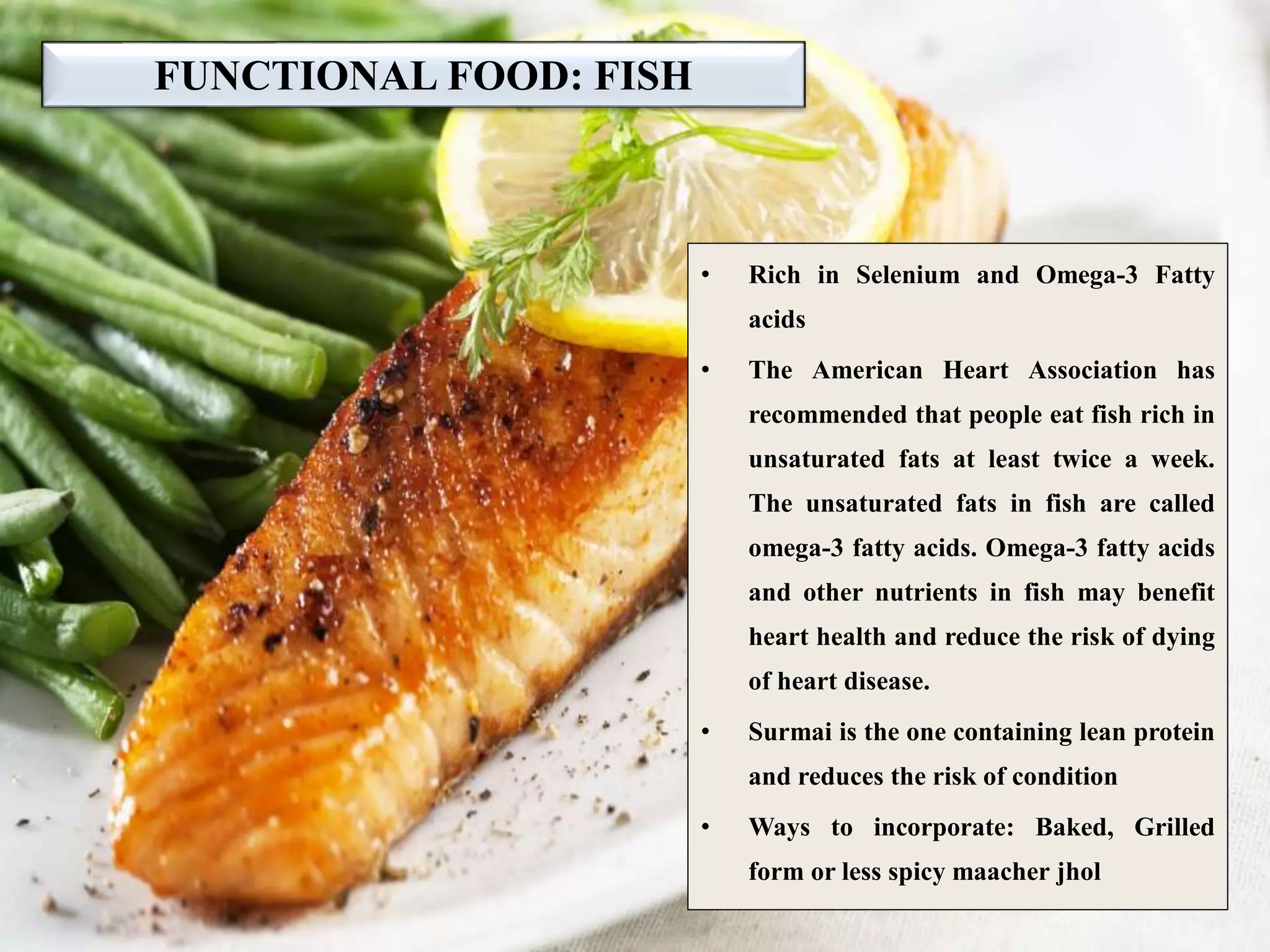
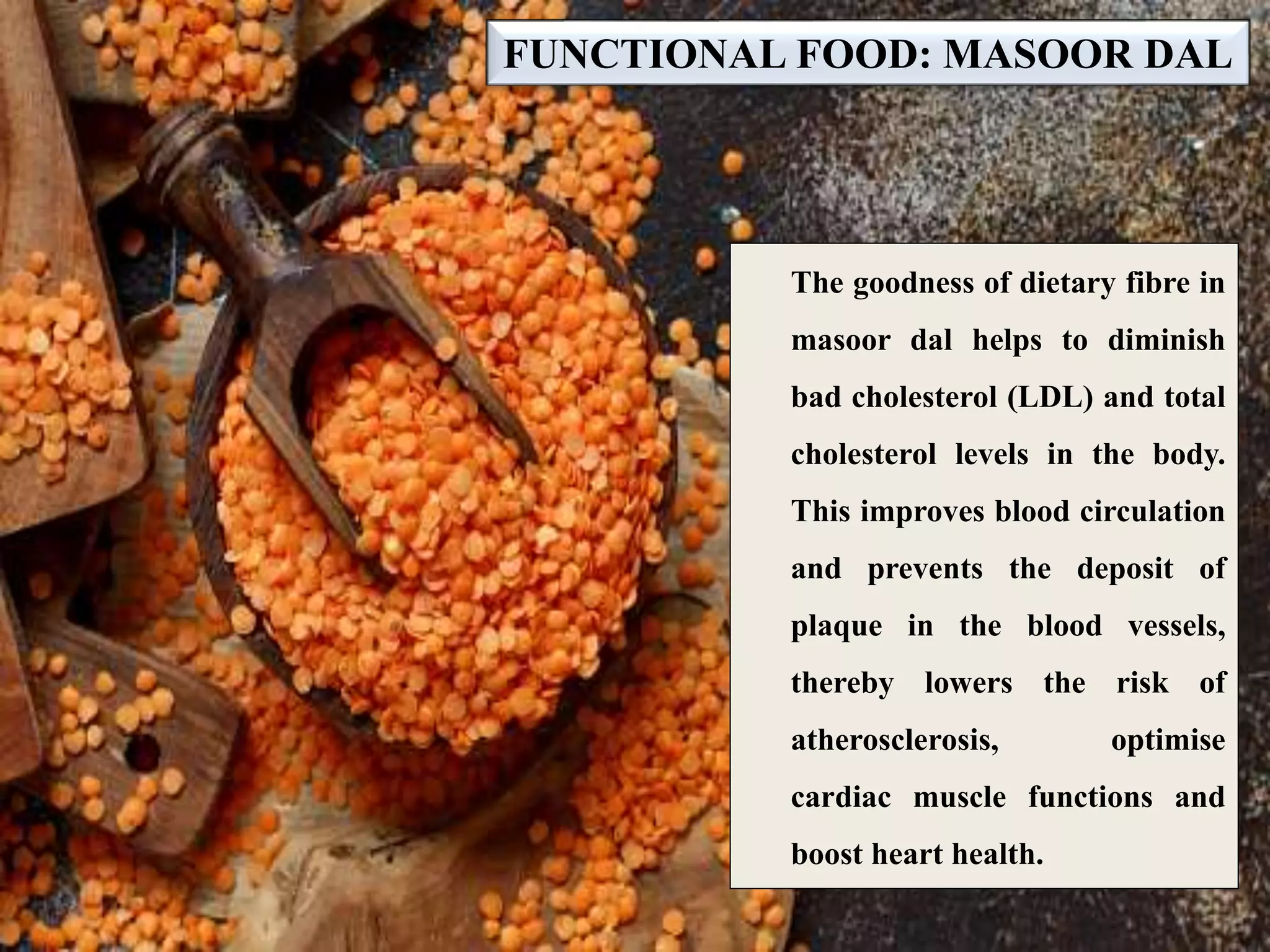
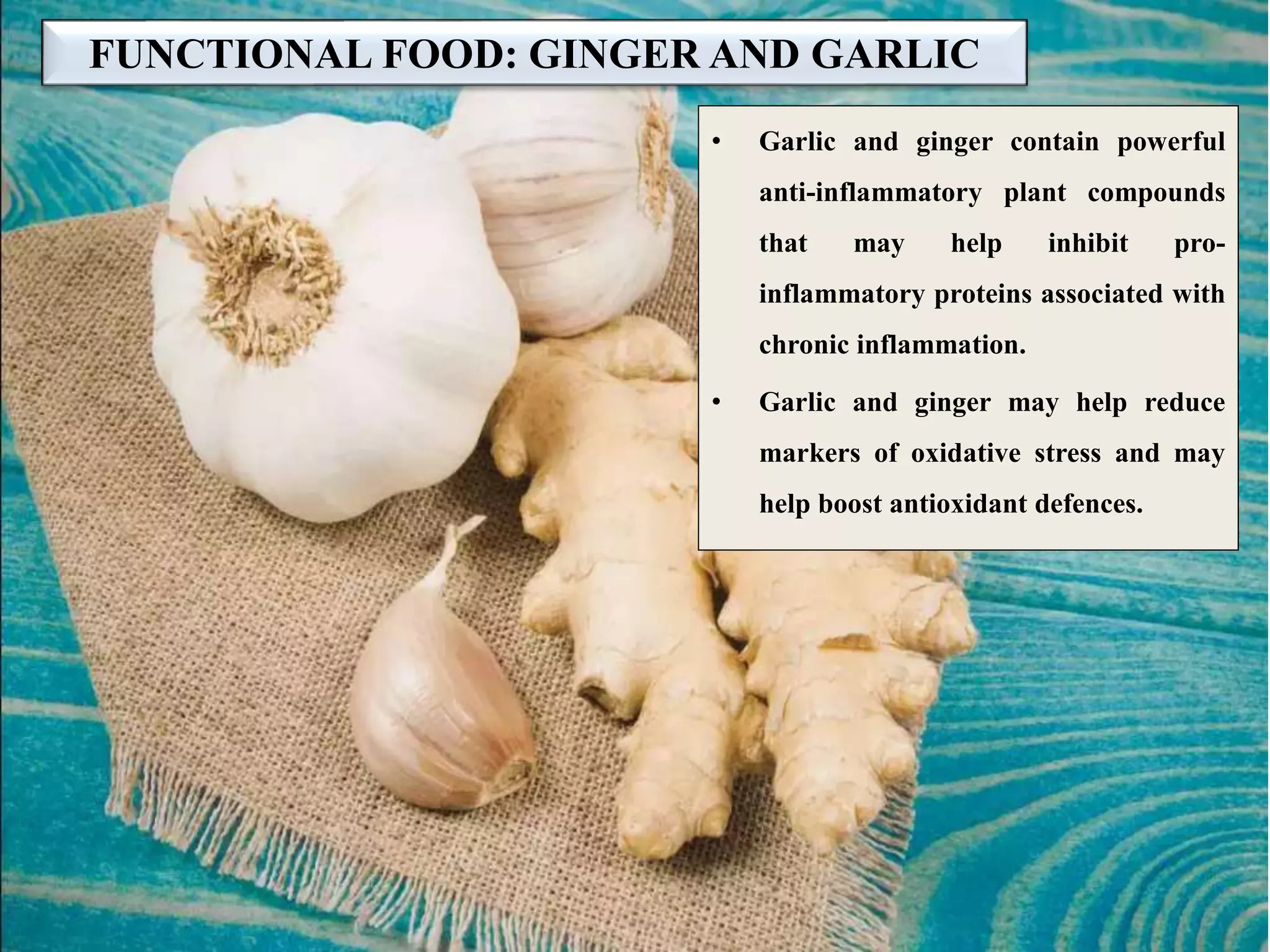
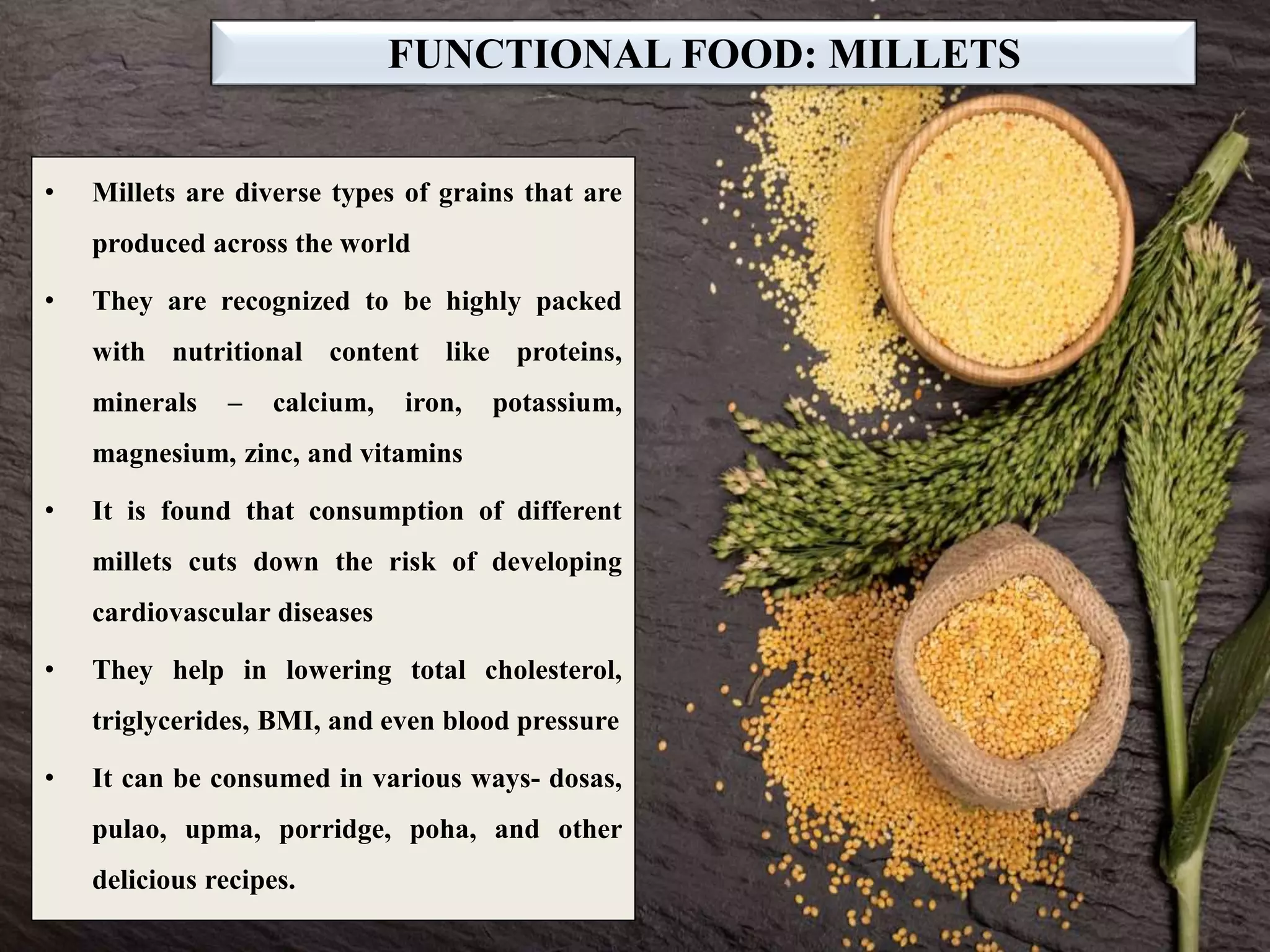






Atherosclerosis is a disease where plaque builds up in the arteries, limiting blood flow. It is caused by chronic inflammation and is the leading cause of heart attacks and strokes. Lifestyle changes like a healthy diet, exercise, weight control, and avoiding tobacco can help prevent and manage atherosclerosis. Functional foods rich in antioxidants, omega-3 fatty acids, fiber and other nutrients may also help reduce the risk and progression of atherosclerosis. These include fish, nuts, citrus fruits, soy, tea, coffee, and cocoa. Proper diagnosis and medical treatment of risk factors like high cholesterol, hypertension, and diabetes are also important to treat atherosclerosis.