


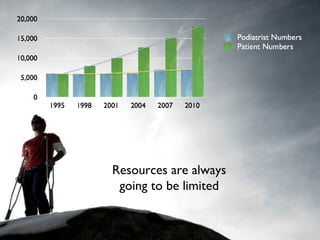
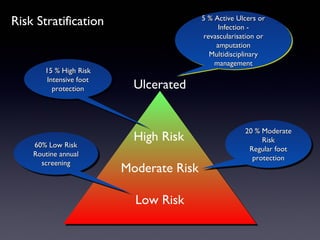
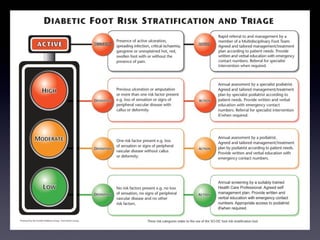
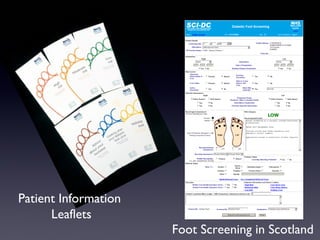



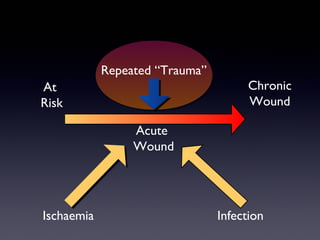
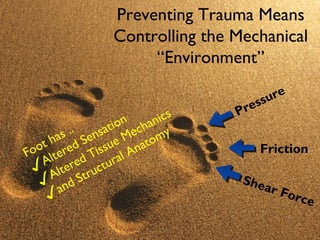















The document discusses the screening, biomechanics, and orthotic management of diabetic foot complications, highlighting the significant burden diabetes places on healthcare systems, with annual costs in the UK reaching approximately £1.8 billion. It emphasizes the importance of effective screening to stratify risk and prevent foot ulcers through tailored interventions, including the use of specialized footwear and orthotic devices. Furthermore, it outlines the mechanical factors contributing to foot ulcers and the necessity of understanding biomechanics in improving treatment outcomes.






























































































