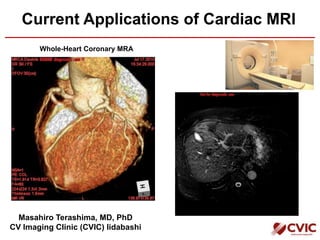


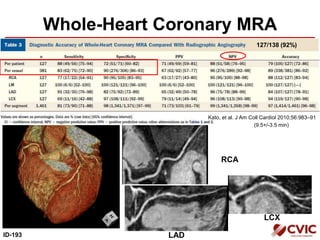
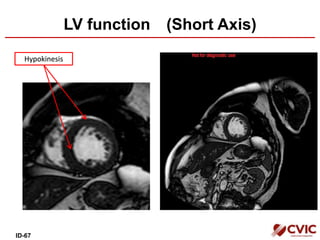



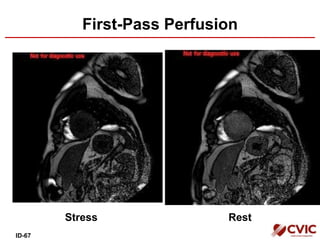
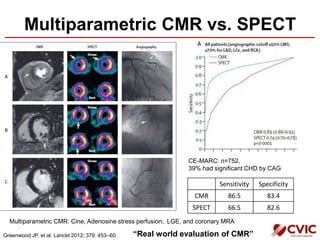

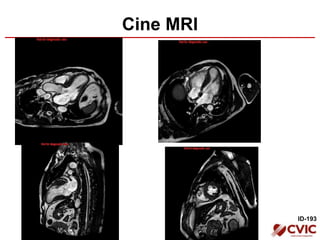


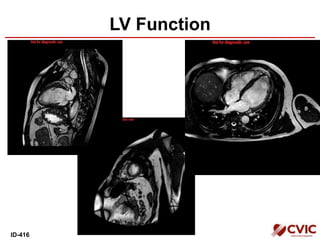



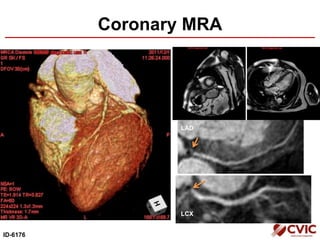



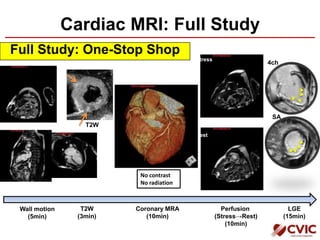

1) Cardiac MRI provides a comprehensive assessment of cardiac structure and function through techniques such as cine imaging, perfusion imaging, late gadolinium enhancement (LGE), and coronary magnetic resonance angiography (MRA) in a single exam without radiation exposure. 2) LGE can identify myocardial scar from prior myocardial infarction (MI), myocarditis, and non-ischemic cardiomyopathies. The detection of unexpected scarring by LGE has important prognostic implications. 3) Combining cardiac CT for assessment of coronary artery calcium with cardiac MRI can help identify patients with prior "unrecognized" MI missed by other testing due to small scars or absence of symptoms.






















































































