Download as PDF, PPTX

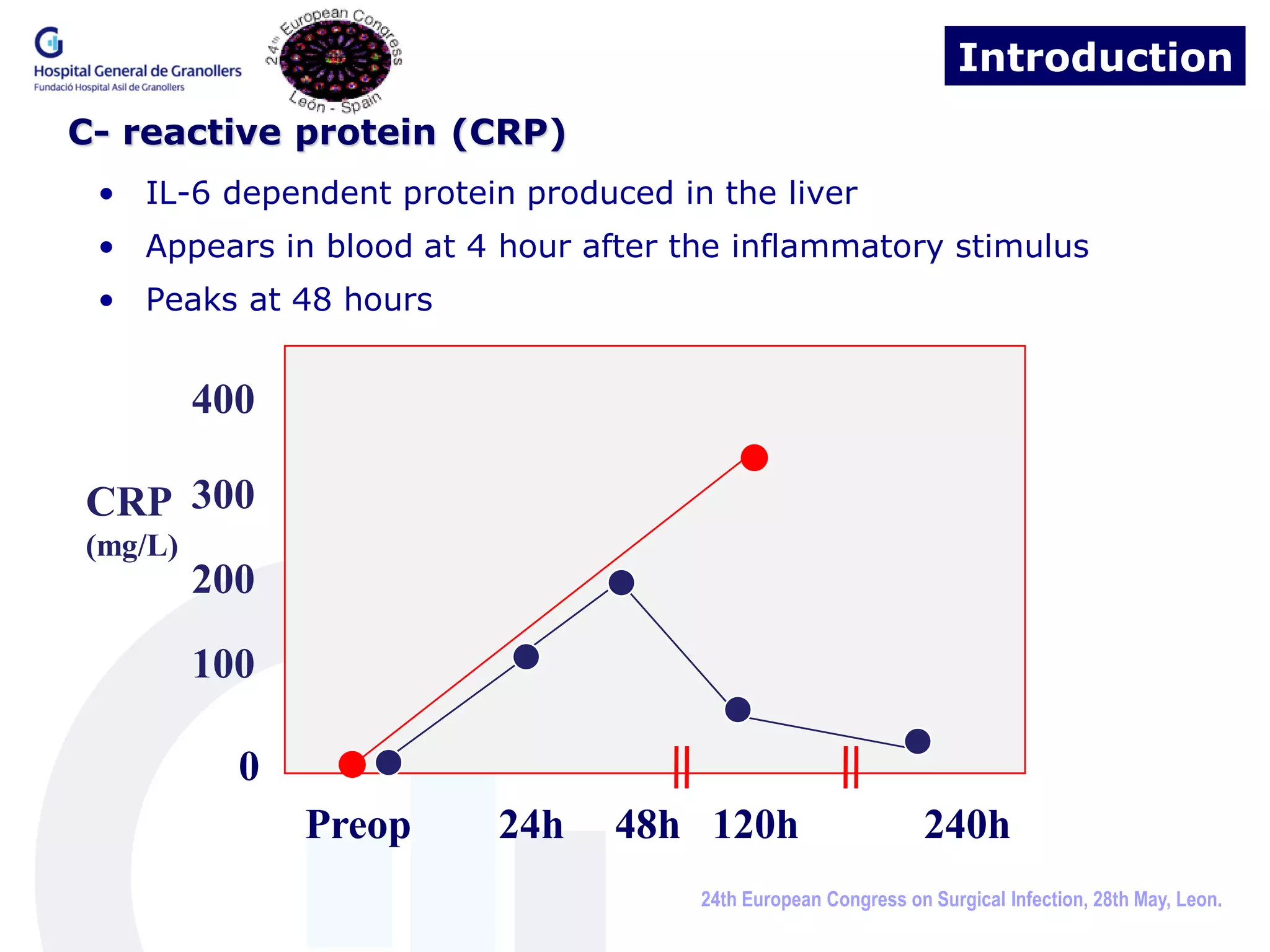

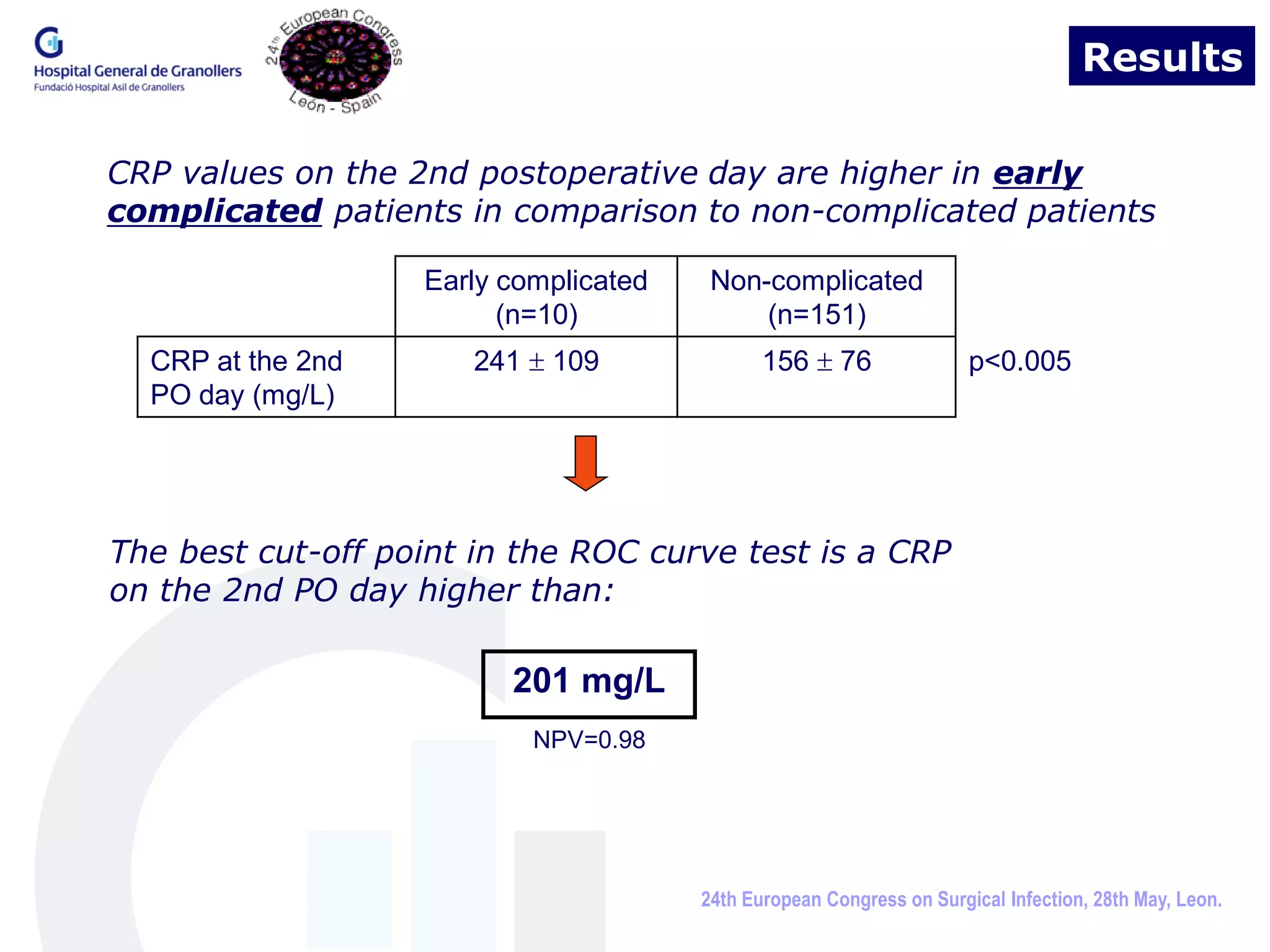
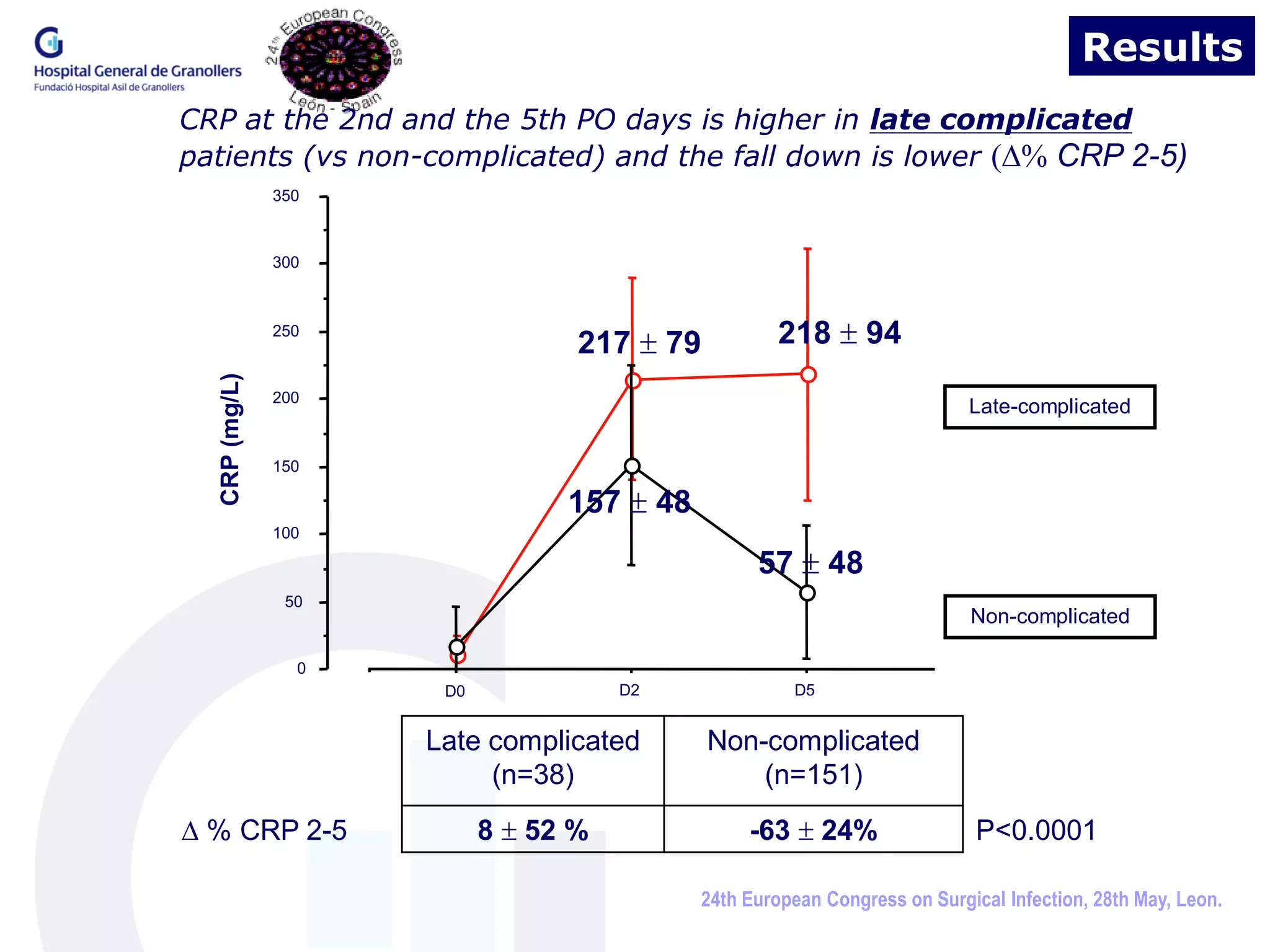
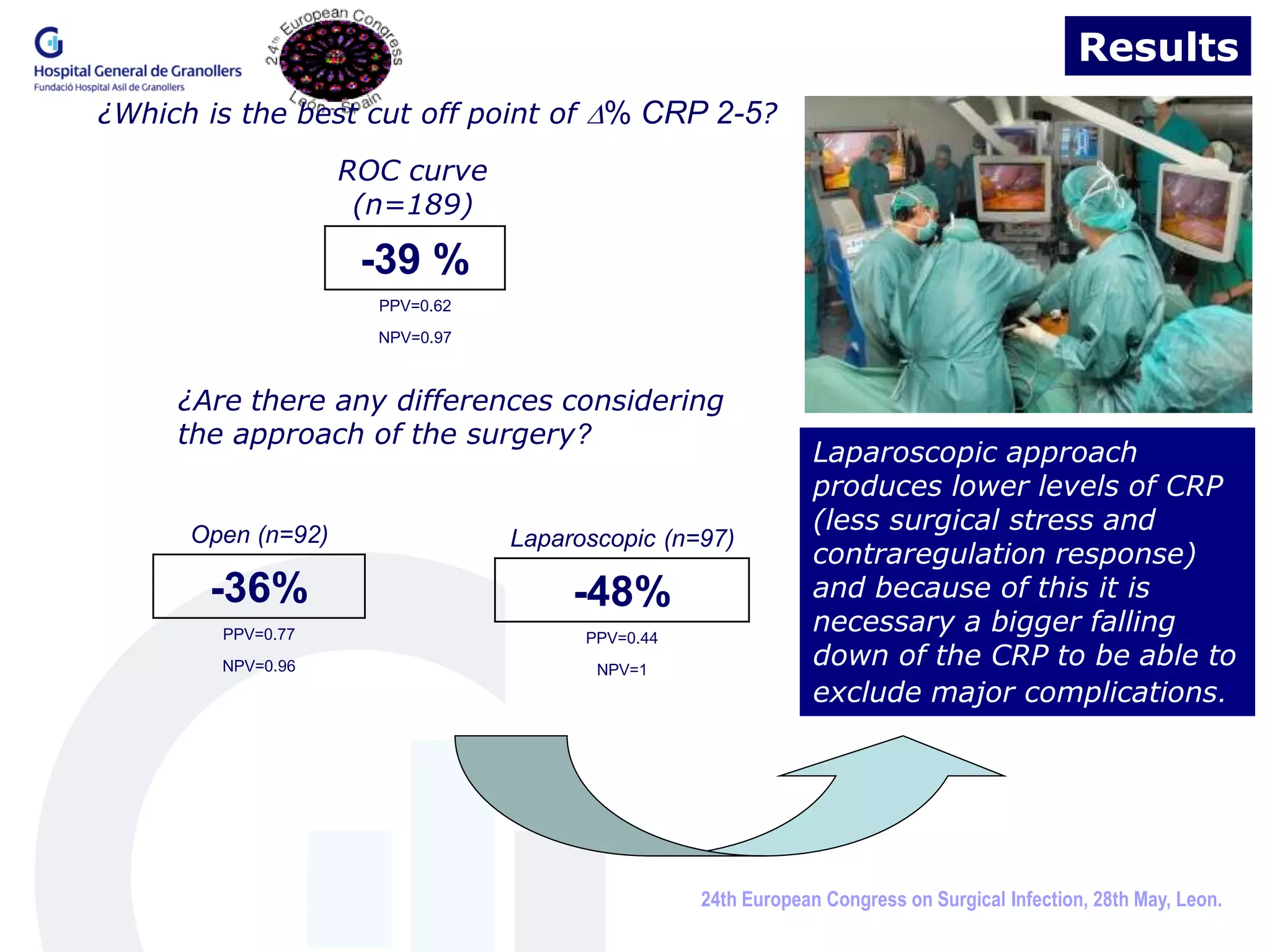


A sufficient decrease in C-reactive protein (CRP) levels after elective colorectal surgery can predict an uneventful recovery. The study found that patients who developed early complications had higher CRP levels on the second postoperative day compared to uncomplicated patients. A decrease in CRP levels between the second and fifth postoperative days of less than 36% for open surgery and 48% for laparoscopic surgery indicated a risk of developing late complications. Monitoring CRP levels in the early postoperative period can help identify patients at risk of septic complications and guide safe discharge from the hospital.














































































