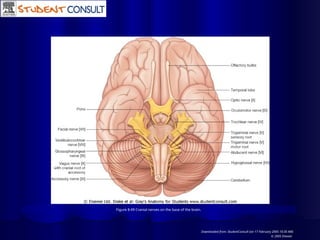
Olfactory nerve
1st
cranialnerve (functional component – SSA)
It is a sensory nerve which carries the sense of smell.
It begins as a dozen of filaments from the olfactory
mucosa of the nasal cavity.
These filaments pass thru the cribriform plate of
ethmoid to reach the olfactory bulb in the anterior
cranial fossa.
Olfactory epithelium of nose --- olfactory rootlets --
Olfactory bulb --Olf. Tract -- lateral and medial
olfact. Stria
Lateral olfact. Stria --Pyriform lobe
Medial olfac. Stria - septal nuclei
Lesions of olfactory nerve result in loss of sense of
smell called anosmia.
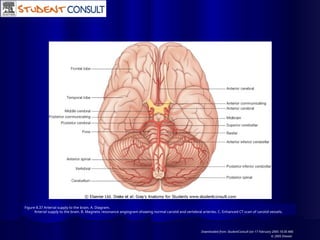
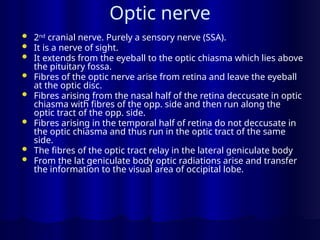
Optic nerve
2nd
cranialnerve. Purely a sensory nerve (SSA).
It is a nerve of sight.
It extends from the eyeball to the optic chiasma which lies above
the pituitary fossa.
Fibres of the optic nerve arise from retina and leave the eyeball
at the optic disc.
Fibres arising from the nasal half of the retina deccusate in optic
chiasma with fibres of the opp. side and then run along the
optic tract of the opp. side.
Fibres arising in the temporal half of retina do not deccusate in
the optic chiasma and thus run in the optic tract of the same
side.
The fibres of the optic tract relay in the lateral geniculate body
From the lat geniculate body optic radiations arise and transfer
the information to the visual area of occipital lobe.
Special features ofoptic nerve
It is not a true peripheral nerve, rather it is a tract of
the forebrain.
It is surrounded by meninges and thus by a
subarachnoid space containing CSF.
Its fibres are myelinated by oligodendrocytes and not
by schwann cells.
Lesion in retina leads to scotoma.
If optic nerve is damaged, there will be complete
blindness on the side of lesion.
Optic chiasma lesion if central leads to bitemporal
hemianopia; but if peripheral on both sides lead to
binasal hemianopia.
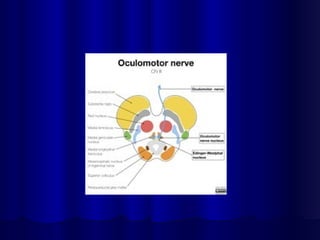
11.
Occulomotor nerve
It isthe 3rd
cranial nerve.
It moves the eyeball.
Supplies most of the muscles of the
eyeball and plays a principal role in
accomodation.
12.
Functional components
Generalsomatic efferent fibres (GSE) : They
arise from the somatic component of
occulomotor nucleus and supply most of the
extrinsic muscles of eyeball.
General visceral efferent (GVE) : They arise
from the parasympathetic component
(Edinger westphal nucleus) of the
occulomotor nucleus. They are preganglionic
parasympathetic fibres that relay in the ciliary
ganglion. The postganglionic fibres from the
ciliary ganglion supply sphincter pupillae and
ciliaris muscle of the eyeball.
13.
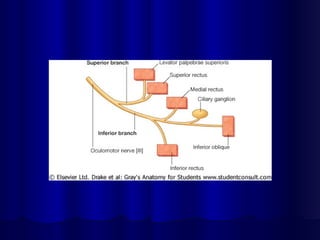
Course of occulomotorN.
It arises from occulomotor nucleus in the midbrain.
The nerve emerges from midbrain in the
interpeduncular fossa, then runs between the
posterior cerebral and superior cerebellar arteries,
pierces the duramater near the apex of petous
temporal bone and travels forward in the lateral wall
of the CS.
In the anterior part of the CS it divides into 2
subdivisions which enter the orbit thru SOF.
The upper division supplies SR and LPS.
The lower division supplies IR, MR and IO muscles of
eyeball. The nerve to IO gives a motor root to the
ciliary ganglion.The post ganglionic fibres from the
ciliary ganglion supply the SP and ciliaris muscles.
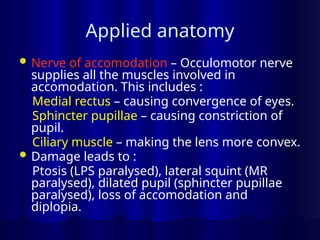
Applied anatomy
Nerveof accomodation – Occulomotor nerve
supplies all the muscles involved in
accomodation. This includes :
Medial rectus – causing convergence of eyes.
Sphincter pupillae – causing constriction of
pupil.
Ciliary muscle – making the lens more convex.
Damage leads to :
Ptosis (LPS paralysed), lateral squint (MR
paralysed), dilated pupil (sphincter pupillae
paralysed), loss of accomodation and
diplopia.
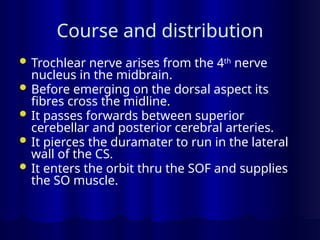
Course and distribution
Trochlear nerve arises from the 4th
nerve
nucleus in the midbrain.
Before emerging on the dorsal aspect its
fibres cross the midline.
It passes forwards between superior
cerebellar and posterior cerebral arteries.
It pierces the duramater to run in the lateral
wall of the CS.
It enters the orbit thru the SOF and supplies
the SO muscle.
Course
It arisesfrom the abducent nucleus in the lower part
of pons and emerges from the brain stem at the
junction of pons and medulla.
It runs upwards, forwards and laterally in the
posterior cranial fossa and crosses dorsal to the
anterior inferior cerebellar artery.
It crosses the petrous tempopral bone to reach the
CS.
It entres the CS by piercing the posterior wall and lies
first lateral and then inferolateral to the ICA.
It enters the orbit thru the SOF and supplies the LR
muscle.
Functional components
GSA –carry exteroceptive sensations
(pain, touch and temperature)from face
and head,mucous membrane of mouth
and nasal cavity.
- proprioceptive sensations muscles of
mastication.
SVE – are motor to muscles of
mastication, anterior belly of digastric,
mylohyoid, tensor palati and tensor
tympani.
32.
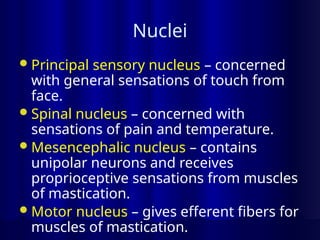
Nuclei
Principal sensory nucleus– concerned
with general sensations of touch from
face.
Spinal nucleus – concerned with
sensations of pain and temperature.
Mesencephalic nucleus – contains
unipolar neurons and receives
proprioceptive sensations from muscles
of mastication.
Motor nucleus – gives efferent fibers for
muscles of mastication.
33.
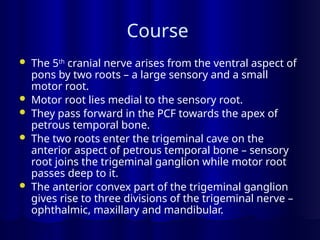
Course
The 5th
cranialnerve arises from the ventral aspect of
pons by two roots – a large sensory and a small
motor root.
Motor root lies medial to the sensory root.
They pass forward in the PCF towards the apex of
petrous temporal bone.
The two roots enter the trigeminal cave on the
anterior aspect of petrous temporal bone – sensory
root joins the trigeminal ganglion while motor root
passes deep to it.
The anterior convex part of the trigeminal ganglion
gives rise to three divisions of the trigeminal nerve –
ophthalmic, maxillary and mandibular.
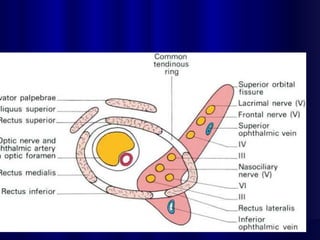
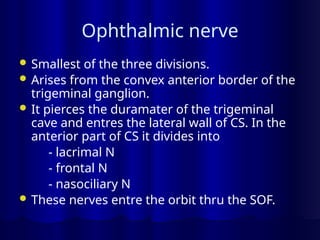
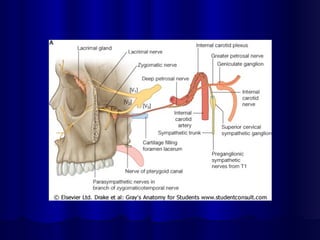
Ophthalmic nerve
Smallestof the three divisions.
Arises from the convex anterior border of the
trigeminal ganglion.
It pierces the duramater of the trigeminal
cave and entres the lateral wall of CS. In the
anterior part of CS it divides into
- lacrimal N
- frontal N
- nasociliary N
These nerves entre the orbit thru the SOF.
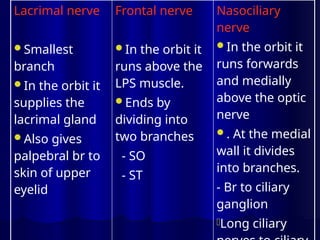
Lacrimal nerve
Smallest
branch
In theorbit it
supplies the
lacrimal gland
Also gives
palpebral br to
skin of upper
eyelid
Frontal nerve
In the orbit it
runs above the
LPS muscle.
Ends by
dividing into
two branches
- SO
- ST
Nasociliary
nerve
In the orbit it
runs forwards
and medially
above the optic
nerve
. At the medial
wall it divides
into branches.
- Br to ciliary
ganglion
-Long ciliary
39.
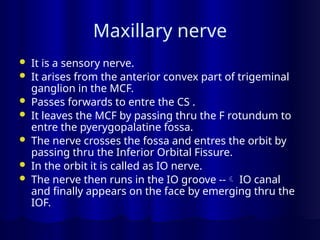
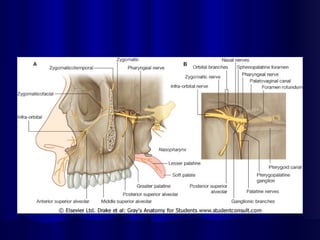
Maxillary nerve
Itis a sensory nerve.
It arises from the anterior convex part of trigeminal
ganglion in the MCF.
Passes forwards to entre the CS .
It leaves the MCF by passing thru the F rotundum to
entre the pyerygopalatine fossa.
The nerve crosses the fossa and entres the orbit by
passing thru the Inferior Orbital Fissure.
In the orbit it is called as IO nerve.
The nerve then runs in the IO groove -- IO canal
and finally appears on the face by emerging thru the
IOF.
40.
Branches (maxillary nerve)
In the MCF – meningeal br
In the PP fossa – ganglionic br (to PP gang.)
- zygomatic br -- divides into ZF & ZT
- posterior superior alveolar (upper molars)
In the orbit – middle superior alveolar (upper
premolars)
- anterior superior alveolar (upper incissors
and canines)
On the face – palpebral (lower lid)
- nasal
- labial (upper lip)
42.
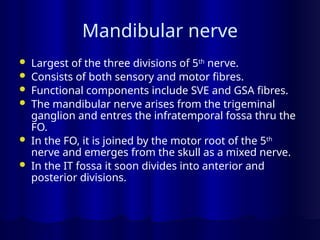
Mandibular nerve
Largestof the three divisions of 5th
nerve.
Consists of both sensory and motor fibres.
Functional components include SVE and GSA fibres.
The mandibular nerve arises from the trigeminal
ganglion and entres the infratemporal fossa thru the
FO.
In the FO, it is joined by the motor root of the 5th
nerve and emerges from the skull as a mixed nerve.
In the IT fossa it soon divides into anterior and
posterior divisions.
43.
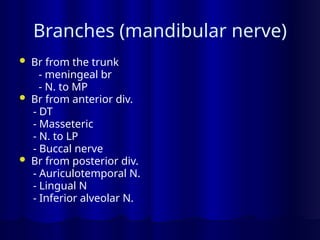
Branches (mandibular nerve)
Br from the trunk
- meningeal br
- N. to MP
Br from anterior div.
- DT
- Masseteric
- N. to LP
- Buccal nerve
Br from posterior div.
- Auriculotemporal N.
- Lingual N
- Inferior alveolar N.
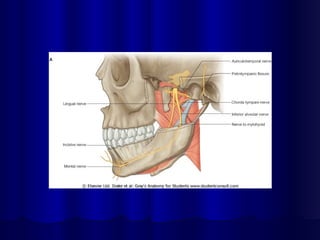
Lingual nerve
It isthe smaller terminal branch of
posterior division. It is sensory to the
mucus membrane of anterior 2/3 of
tongue. In its course it is closely related
to third molar and near its termination
to the submandibular duct.
Applied anatomy - Lingual nerve is at
great risk during the surgical removal of
impacted third molar tooth.
47.
The nerve isat risk during removal of
the submandibular gland, during which
the submandibular duct must be
dissected out carefully.
48.
Inferior alveolar nerve
Oneof the terminal br of posterior div.
of mandibular nerve.
It runs vertically downwards lateral to
medial pterygoid.
It entres the mandibular foramen and
runs in the mandibular canal.
Branches (inferior alveolarN.)
Mylohyoid br. ( supplies the mylohyoid
M. and ant. Belly of digastric)
Dental br – to molars and premolars.
Insicive br – canine and incisor teeth.
Mental nerve – emerges at the mental
foramen and supplies skin of the chin
and lower lip.
51.
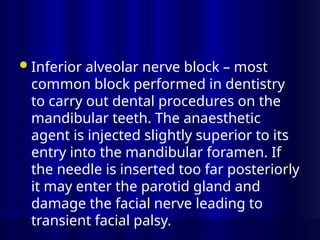
Inferior alveolar nerveblock – most
common block performed in dentistry
to carry out dental procedures on the
mandibular teeth. The anaesthetic
agent is injected slightly superior to its
entry into the mandibular foramen. If
the needle is inserted too far posteriorly
it may enter the parotid gland and
damage the facial nerve leading to
transient facial palsy.
52.
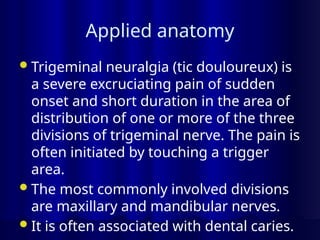
Applied anatomy
Trigeminal neuralgia(tic douloureux) is
a severe excruciating pain of sudden
onset and short duration in the area of
distribution of one or more of the three
divisions of trigeminal nerve. The pain is
often initiated by touching a trigger
area.
The most commonly involved divisions
are maxillary and mandibular nerves.
It is often associated with dental caries.
53.
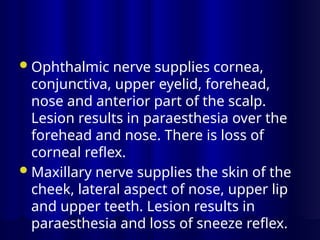
Ophthalmic nerve suppliescornea,
conjunctiva, upper eyelid, forehead,
nose and anterior part of the scalp.
Lesion results in paraesthesia over the
forehead and nose. There is loss of
corneal reflex.
Maxillary nerve supplies the skin of the
cheek, lateral aspect of nose, upper lip
and upper teeth. Lesion results in
paraesthesia and loss of sneeze reflex.
55.
Mandibular nerve providessensory
innervation to the skin over the
mandible, auricle, lower lip and teeth.
Lesion results in paraesthesia along the
mandible and lower teeth and loss of
jaw jerk.
Referred pain – It is the pain referred
from one br of the mandibular nerve to
the other. The pain of tongue cancer
(lingual nerve) is referred to the
56.
Frey’s syndrome –It is a complication
that occurs when AT and Gr Auricular
nerves are cut by a wound or incision in
the parotid region.
When the patient eats beads of
prespiration appears on the face in the
parotid region. When the fibers of the
above nerves are cut , during the
process of regeneration the
parasympathetic secretomotor fibers of
57.
- destined tosupply the parotid gland
grow out and join the fibers of the Gr.
Auricular nerve meant to supply the
sweat glands. When the person eats
stimulus intended for saliva production,
produces sweat secretion instead.

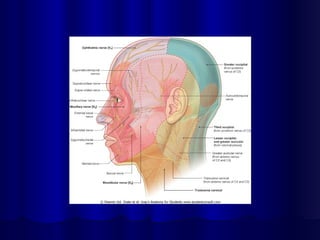
![Figure 8.97 Ophthalmic nerve [V1] and its divisions.
Downloaded from: StudentConsult (on 17 February 2005 10:50 AM)
© 2005 Elsevier](https://image.slidesharecdn.com/cranialnerves1-250409013004-9ffa0779/85/cranial-nerves-1anantomypresentatio-pptx-7-320.jpg)

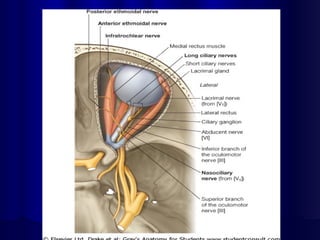

![Figure 8.98 Relationship of the ophthalmic nerve [V1] and its divisions to the muscles of the eyeball.
Downloaded from: StudentConsult (on 17 February 2005 10:50 AM)
© 2005 Elsevier](https://image.slidesharecdn.com/cranialnerves1-250409013004-9ffa0779/85/cranial-nerves-1anantomypresentatio-pptx-36-320.jpg)
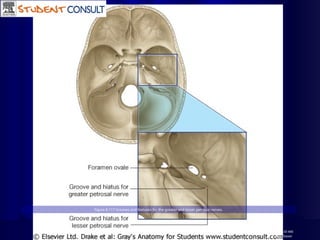
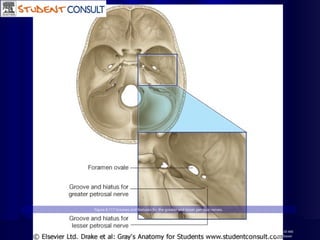
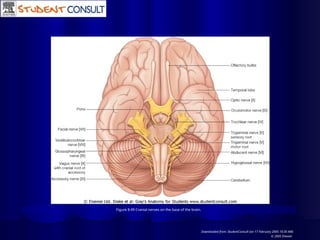
![Figure 8.58 Trigeminal nerve [V] leaving the skull.
Downloaded from: StudentConsult (on 17 February 2005 10:49 AM)
© 2005 Elsevier](https://image.slidesharecdn.com/cranialnerves1-250409013004-9ffa0779/85/cranial-nerves-1anantomypresentatio-pptx-45-320.jpg)
![Figure 8.139 Mandibular nerve [V3]-posterior trunk. A. Lateral view.
Mandibular nerve [V3]-posterior trunk. B. Anterior view. C. Anteromedial view.
Downloaded from: StudentConsult (on 17 February 2005 11:10 AM)
© 2005 Elsevier](https://image.slidesharecdn.com/cranialnerves1-250409013004-9ffa0779/85/cranial-nerves-1anantomypresentatio-pptx-49-320.jpg)









































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)





