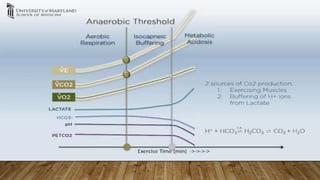
CPET, or cardiopulmonary exercise testing, is the gold standard for assessing functional capacity in heart failure patients. It combines ECG stress testing with measurements of gas exchange and ventilation. Key parameters measured include oxygen uptake, carbon dioxide production, minute ventilation, heart rate, and oxygen saturation. CPET can help determine if exercise limitation is due to pulmonary, cardiovascular, or peripheral causes by measuring values like oxygen pulse and the ventilatory threshold. It has several clinical applications for evaluating unexplained dyspnea, monitoring disease progression, and preoperative risk assessment.