Download to read offline

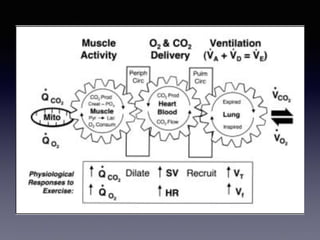
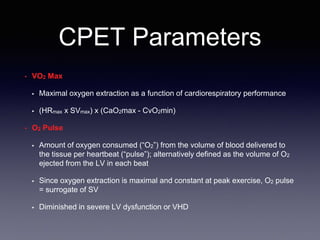


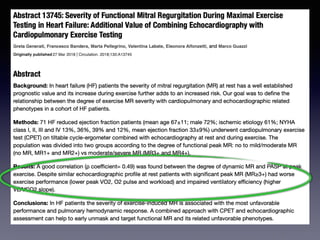
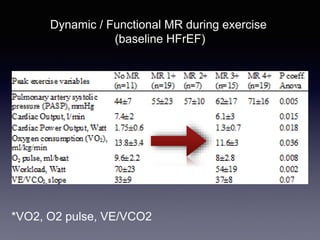
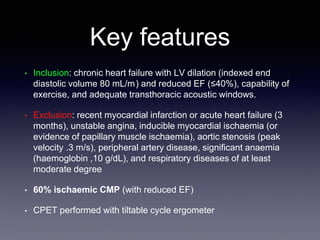

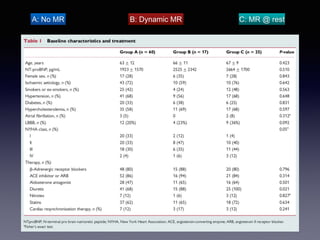

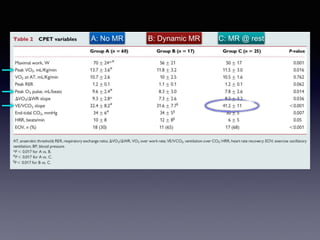
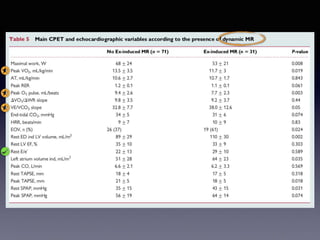









The document discusses the use of cardiopulmonary exercise testing (CPET) in evaluating functional capacity in patients with mitral regurgitation, focusing on various CPET parameters such as VO2 max, O2 pulse, and ventilatory efficiency. It highlights correlations between exercise performance and mitral regurgitation severity, noting that impaired ventilatory efficiency is significant in patients with severe conditions. The study emphasizes the importance of rehabilitation in managing these patients.














































































