Downloaded 33 times

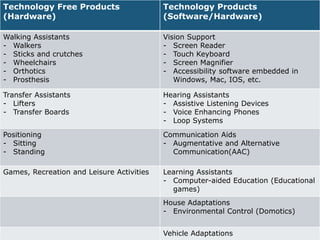
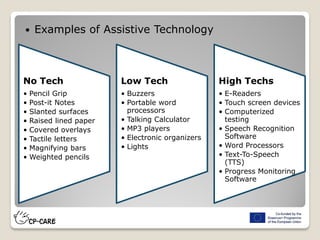
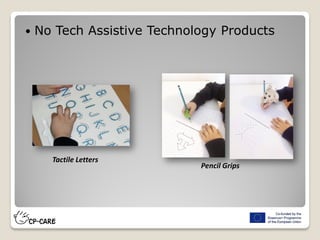


























The document discusses assistive technology for individuals with cerebral palsy, detailing various devices and systems that support mobility, communication, and daily activities. It covers categories of technology, including no-tech, low-tech, and high-tech solutions, as well as specific aids for different bodily functions. Additionally, it emphasizes the importance of tailored adaptive equipment to enhance the independence and quality of life for users.























































































