Downloaded 36 times
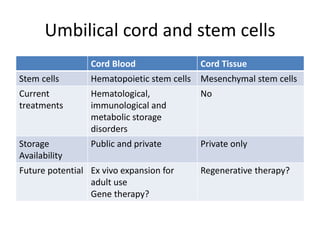
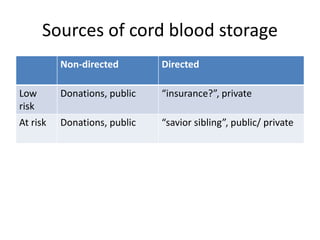
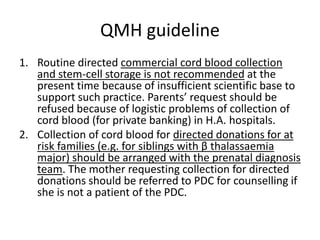
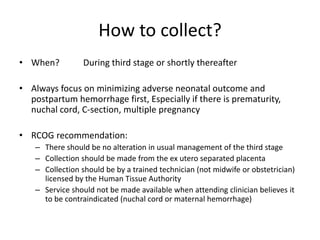
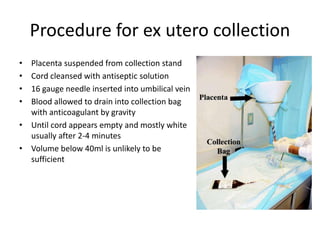

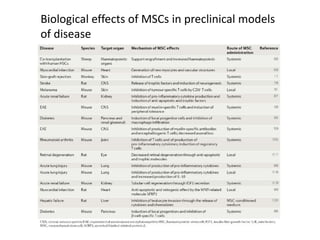


Cord blood storage and stem cells offers potential clinical applications. In Hong Kong, public cord blood banking is available through the Red Cross while private storage options exist. Cord blood contains hematopoietic stem cells currently used to treat blood and immune disorders. Larger quantities of stem cells can be obtained through cord tissue. Mesenchymal stem cells show promise for regenerative therapies in neurological and cardiac conditions but require more research. Guidelines recommend no alteration of normal delivery for cord blood collection and processing within 48 hours.





























































![Hypothalamus short ppt by Dr. Neha [PT].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/hypothalamusbydr-260124145759-b9f94a93-thumbnail.jpg?width=640&height=640&fit=bounds)


















