This document discusses several diseases associated with pregnancy, including their definitions, effects, diagnosis, and management. It summarizes:
1) Anemia is common in pregnancy due to increased iron needs. It can cause complications for both mother and baby if not treated with iron supplementation.
2) Cardiac diseases can be exacerbated by the increased demands of pregnancy. Management involves monitoring, activity restriction, and optimizing delivery to reduce stress.
3) Malaria and tuberculosis infections become more severe and common during pregnancy. Both require prompt treatment to prevent maternal and fetal complications.
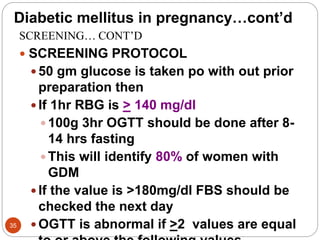
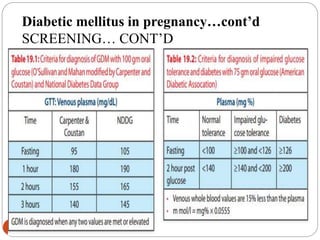
4) Gestational diabetes develops in some pregnancies due to insulin resistance and higher blood sugar levels. Close monitoring and treatment are needed to