Downloaded 318 times

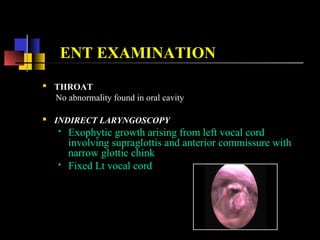
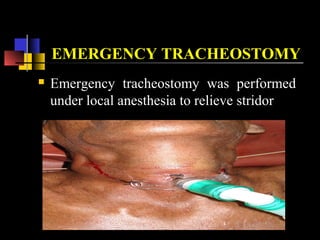
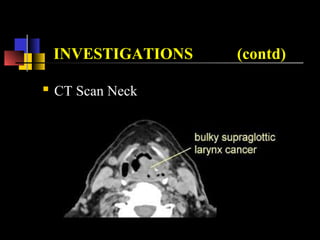
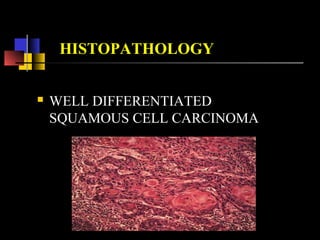





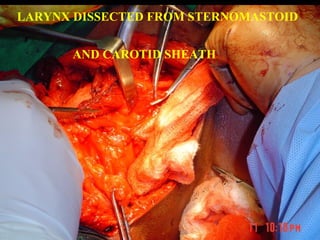



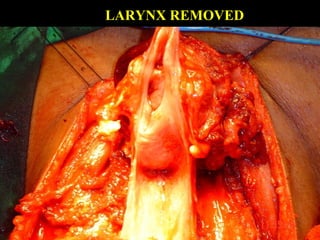

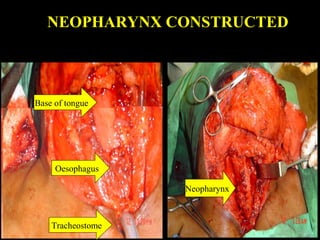

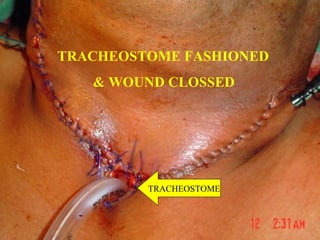
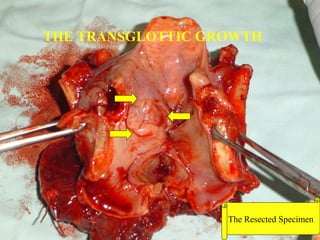


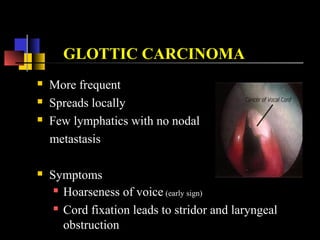
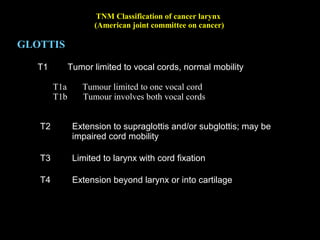


This document describes a case of carcinoma of the larynx in a 65-year-old male patient who presented with hoarseness of voice for 6 months and breathing difficulty for 2 weeks. Examination revealed a growth on the left vocal cord. The patient underwent an emergency tracheostomy followed by a total laryngectomy and biopsy, which showed well-differentiated squamous cell carcinoma. The patient recovered well post-operatively and was discharged on adjuvant radiotherapy and voice rehabilitation.











































































































