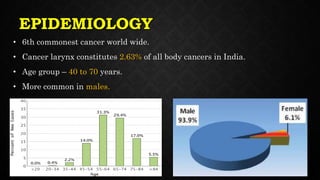
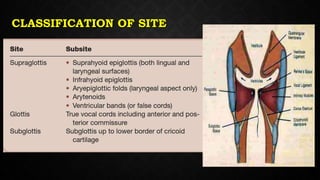
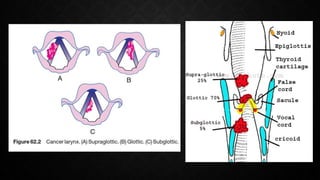
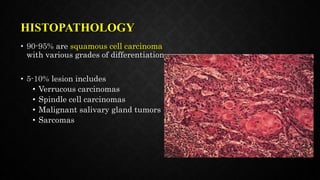
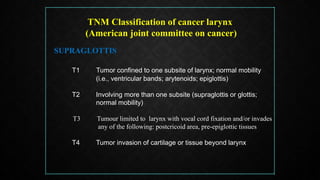
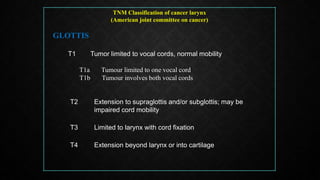
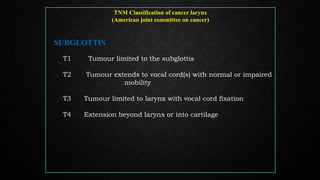
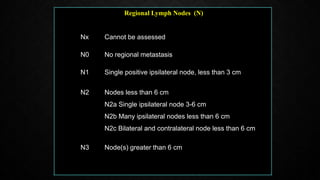
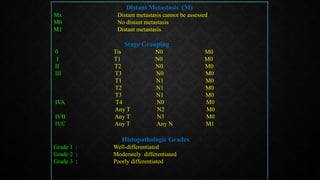
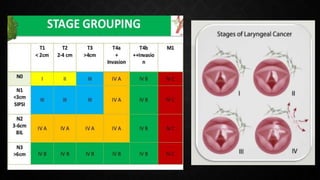
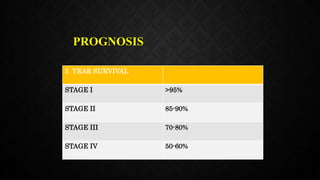
Carcinoma of the larynx is the 6th most common cancer globally, accounting for 2.63% of all body cancers in India, mainly affecting males aged 40 to 70 years, with notable risk factors including tobacco, alcohol, and environmental exposures. Most laryngeal cancers are squamous cell carcinomas, and the disease is classified using the TNM system to determine stages and treatment options, including surgery, radiotherapy, and combined therapies. Prognosis varies by stage, with a 5-year survival rate of over 95% in stage I and decreasing to 50-60% in stage IV, emphasizing the importance of early diagnosis and intervention.



































































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)









