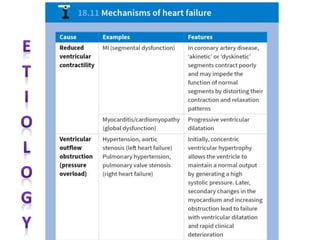
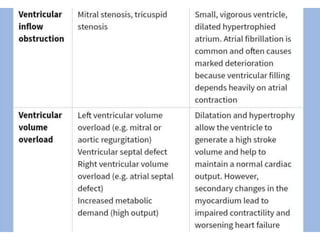
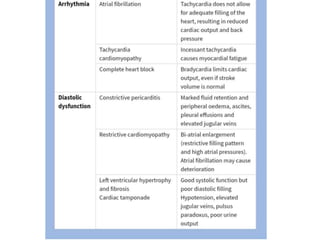
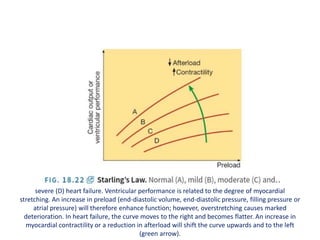
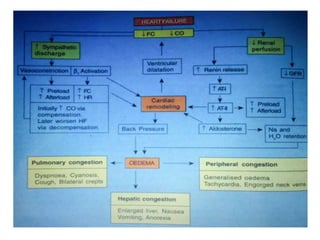
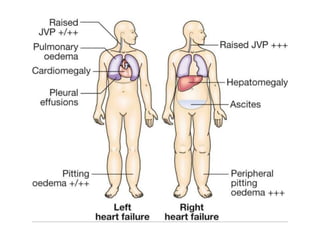
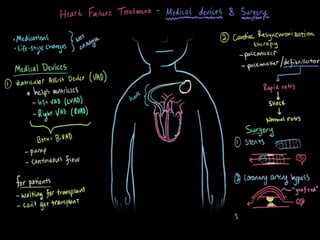
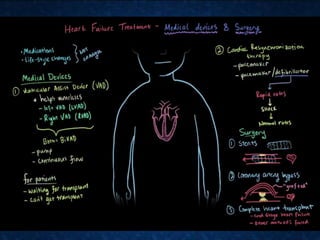
This document provides information on congestive cardiac failure (CCF), including its definition, pathophysiology, clinical features, investigations, and management. CCF occurs when the heart muscle is weakened and cannot maintain adequate cardiac output. The pathophysiology involves changes in preload, afterload, and contractility that decrease cardiac output. Compensatory mechanisms initially help but later worsen symptoms. Clinically, CCF presents with dyspnea, edema, elevated JVP, hepatomegaly, and other signs. Investigations include BNP, ECG, echocardiogram. Management focuses on treating the underlying cause, reducing preload/afterload, and improving contractility. Diuretics, ACE inhibitors, beta