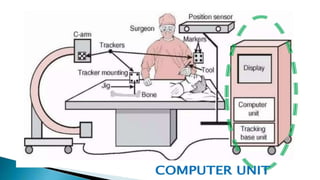
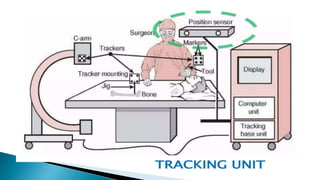
Computer-assisted orthopaedic surgery (CAOS) leverages computer technology for enhanced accuracy in surgical procedures, including preoperative planning and intraoperative navigation. The document details various components and technologies involved in CAOS, such as tracking systems, smart tools, and robotic assistance, as well as their applications in hip and knee arthroplasties and spinal stabilization. Additionally, it addresses potential complications and challenges in navigation procedures and emphasizes the advantages of robotic surgery in terms of precision and minimal invasiveness.