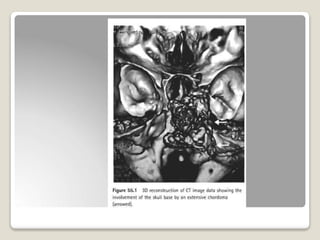
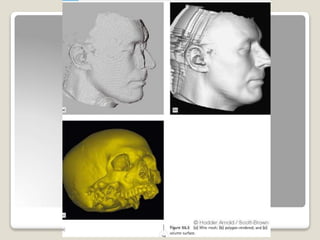
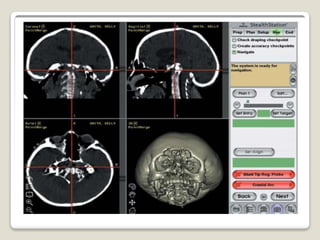
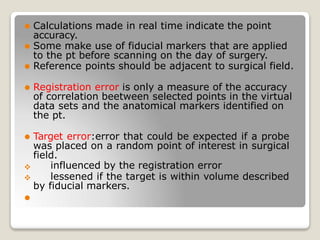
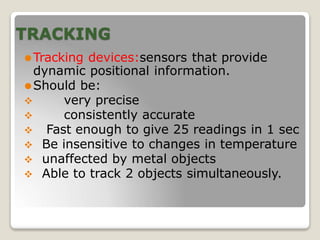
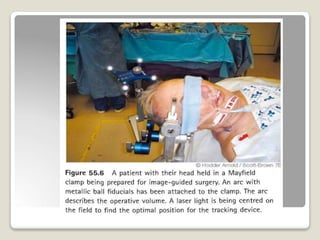
The document discusses image-guided surgery and its advancements in various fields, including neurosurgery and orthopaedics, due to developments in computer science and imaging technology. It explains the use of 3D imaging for surgical planning, navigation, and simulation, enhancing surgical accuracy and efficiency while reducing risks and operative times. It also details the processes of image reconstruction, registration, tracking, and clinical applications in surgeries such as skull base and endoscopic procedures.












































![Virtual surgery [new].ppt](https://cdn.slidesharecdn.com/ss_thumbnails/finalppt-111113045537-phpapp01-thumbnail.jpg?width=640&height=640&fit=bounds)






































