
Recommended
More Related Content
Similar to Coma_.pptx
Similar to Coma_.pptx (20)
More from DrSachinPandey2
More from DrSachinPandey2 (20)
Recently uploaded
Recently uploaded (20)
Coma_.pptx
- 2. Definitions Coma is defined as a state of unresponsiveness and unconsciousness Coma from the Greek word "koma," meaning deep sleep Coma can be a medical emergency That requires intervention without always knowing the cause Knowledge of CNS anatomy can give clues to the cause
- 3. Definitions of levels of arousal ((conciousness Alert (Conscious) - Appearance of wakefulness, awareness of the self and environment Lethargy - mild reduction in alertness Obtundation - moderate reduction in alertness. Increased response time to stimuli. Delirium -disturbed consciousness with motor restlessness, disorientation and hallucination
- 4. Definitions of levels of arousal ((Consciousness Stupor - Deep sleep, patient can be aroused only by vigorous and repetitive stimulation. Returns to deep sleep when not continually stimulated. Coma (Unconscious) - Sleep like appearance and behaviorally unresponsive to all external stimuli (Unarousable unresponsiveness, eyes closed)
- 5. Encephalopathy Encephalopathy describes a diffuse disorder of the brain in which at least two of the following symptoms are present: (1)altered states of consciousness, (2)altered cognition or personality, and (3)seizures. Encephalitis is an encephalopathy accompanied by cerebrospinal fluid (CSF) pleocytosis.
- 6. locked-in syndrome a brainstem disorder in which the individual can process information but cannot respond .
- 7. Persistent Vegetative State PVS PVS is a form of eyes-open permanent unconsciousness after recovery from coma with loss of cognitive function and awareness of the environment but preservation of sleep-wake cycles and vegetative function. Survival is indefinite with good nursing care. The usual causes, in order of frequency, are anoxia and ischemia, metabolic or encephalitic coma, and head trauma. Anoxia-ischemia has the worst prognosis. Children who remain in a PVS for 3 months do not regain functional skills.
- 8. Glasgow Coma Scale GCS Developed to define outcome in adult patients with head injury Coma: score of 8 or less There is a modified scale used for infants and children
- 9. Glasgow Score Eye opening Motor Response Spontaneous 4 obeys commands 6 To command 3 localizes pain 5 To pain 2 withdraws to pain 4 None 1 abnormal flexion 3 Verbal abnormal extension 2 Oriented 5 none 1 Confused 4 Inappropriate words 3 TOTAL 3-15 Incomprehensible sounds 2 None 1
- 10. MODIFIED GLASGOW COMA SCORE For Infants Eye opening Motor 6 spontaneous 4 normal To speech 3 withdraws to touch 5 To pain 2 withdraws to pain 4 3 None 1 abnormal flexion Verbal abnormal extension 2 1 Coos 5 none Irritable cries 4 Cries to pain 3 Moans to pain 2 None 1
- 11. GCS Individual elements as well as the sum of the score are important. The score is expressed in the form "GCS 9 = E2 V4 M3 at 07:35 Generally, coma is classified as: Severe, with GCS ≤ 8 Moderate, GCS 9 - 12 Minor, GCS ≥ 13.
- 12. Causes of COMA
- 13. Causes of Impaired Consciousness Possible Causes Alcohol Epilepsy nsulin, Intoxication Insulin, Intoxication Overdose Uremia (and other metaboliccauses) Trauma Infection Psychiatric Stroke, Syncope AEIOU TIPS
- 14. Epileptic Absence status Complex partial seizure Post epileptic depression
- 15. Hypoxia-ischemia Shock Cardiac or pulmonary failure (Cardiac arrest, arrhythmia, CHF) Near drowning Carbon monoxide poisoning Strangulation
- 16. Hypoxia and Ischemia Hypoxia and ischemia usually occur together acute anoxia results in immediate loss of consciousness. Prolonged hypoxia causes personality change first, then loss of consciousness; Prolonged hypoxia can result from severe anemia (oxygen-carrying capacity reduced by at least half), congestive heart failure, chronic lung disease, and neuromuscular disorders.
- 17. Diagnosis. Cerebral edema is prominent during the first 72 hours after severe hypoxia. CT during that time shows decreased density with loss of the differentiation between gray and white matter. Severe, generalized loss of density on the CT scan correlates with a poor outcome. An EEG that shows a burst-suppression pattern or absence of activity is associated with a poor neurological outcome or death.
- 18. BURST SUPRESSION pattern of burst of slow and mixed waves often of high amplitude alternating with a flat baseline. It is usually seen after severe brain injury such as post ischemia or post anoxia
- 19. Maintaining oxygenation, circulation, and blood glucose concentration is essential. (hyperventilation) Regulate intracranial pressure to levels that allow satisfactory cerebral perfusion Anticonvulsant drugs manage seizures Anoxia is invariably associated with lactic acidosis. Restoration of acid-base balance is essential. barbiturate coma to slow cerebral metabolism is common practice . Hypothermia prevents brain damage during the time of hypoxia and ischemia but has questionable value after the event. Corticosteroids do not improve neurological recovery in patients with global ischemia after cardiac arrest.
- 20. Causes of Impaired Consciousness .cont STRUCTURAL TRAUMA NEOPLASMS VASCULAR DISEASE FOCAL INFARCTION HYDROCEPHALUS Stroke
- 21. Infectious Causes of Coma Bacterial meningitis Brain abscess Epidural, subdural empyema Fungal meningitis Viral encephalitis Postinfectious encephalomyelitis ADEM
- 22. Viral encephalitis Enteroviruses and herpes simplex virus (HSV) are now the most common viral causes of encephalitis in children. Specific viral identification is possible, however, in only 15% to 20% of cases. In addition to viruses that directly infect the brain and meninges, encephalopathies may follow systemic viral infections. These probably result from demyelination caused by immune- mediated responses of the brain to infection.
- 23. Acute disseminated encephalomyelitis ((ADEM Immune-mediated disease of brain. It usually occurs following a viral infection or vaccination, but it may also appear spontaneously. Abrupt onset and a monophasic course. Symptoms usually begins 1-3 weeks after infection or vaccination. Major symptoms are fever, headache, drowsiness, seizures and coma.
- 24. BRAIN ABSCESS
- 25. Trauma Concussion Cerebral contusion Epidural hematoma Subdural hematoma/effusion Intracerebral hematoma
- 26. Parenchymal haemorrhage May cause a rapid decline in consciousness, from 1. Rupture into the ventricles 2. or subsequent herniation and brainstem compression. Cerebellar haemorrhage or infarct with 1. Subsequent oedema 2. Direct brainstem compression, early decompression can be lifesaving.
- 27. Lt frontoprietal intracerebral he (hyperdense( (Massive (midline shift
- 28. Multifocal hematoma , lt fronal & temporal
- 30. Rt frontoparietal epidural hematoma +cephalohematoma
- 31. SUBDURAL HEMATOMA Subdural bleeding due to tearing of veins
- 32. Hgh in lateral ventricles + dilated ventricles
- 33. Metabolic Disorders The inborn errors of metabolism that cause states of decreased consciousness are usually associated with hyperammonemia, hypoglycemia, or organic aciduria. Neonatal seizures are an early feature in most of these conditions, but some may not cause symptoms until infancy or childhood. Hypoglycemia Acidosis Hyperammonemia Uremia
- 34. Inborn errors with a delayed onset of encephalopathy include disorders of pyruvate metabolism and respiratory chain disorders ,glycogen storage diseases , and primary carnitine deficiency. DKA ( diabetic Ketoacidosis) Hepatic coma Hypernatremia The usual causes Dehydration or overhydration with hypertonic saline solutions. Hypernatremia is a medical emergency and, if not corrected promptly, may lead to permanent brain damage and death.
- 35. Hyponatremia Hyponatremia may result from water retention, sodium loss, or both. The syndrome of inappropriate antidiuretic hormone secretion (SIADH) is an important cause of water retention. Sodium loss results from renal disease, vomiting, and diarrhea. Permanent brain damage from hyponatremia is uncommon but may occur in otherwise healthy children if the serum sodium concentration remains less than 115 mEq/L for several hours.
- 36. Renal coma May occur in acute or chronic renal failure Raised blood urea alone cannot be responsible for the loss of consciousness but the Metabolic acidosis, electrolyte disturbances and Water intoxication due to fluid retention may be responsible Toxic Causes Immunosuppressive drugs Substance abuse Toxins
- 38. History and Physical Examination Obtain a careful history of the following: (1)the events leading to the behavioral change; (2)drug or toxic exposure (prescription drugs are more often at fault than substances of abuse, and a medicine cabinet inspection should be ordered in every home the child has visited); (3)a personal or FH of migraine or epilepsy; (4)recent or concurrent fever, infectious disease, or systemic illness (5)a previous personal or family history of encephalopathy.
- 39. General Physical Exam The important variables in locating the site of abnormality are state of consciousness, pattern of breathing, pupillary size and reactivity, eye movements, and motor responses. The cause of lethargy and obtundation is usually mild depression of hemispheric function. Stupor and coma are characteristic of much more extensive disturbance of hemispheric function or involvement of the diencephalon and upper brainstem. Vital signs Fever (may mean infection) Very high temperature and dry skin – consider heat stroke Hypothermia often seen in drug intoxication BP
- 40. Skin examination Cyanosis Cherry red - carbon monoxide (almond odor) Café au lait spots - neurofibromatosis Shagreen patches - tuberous sclerosis Hyperpigmentation - Addison disease Petechiae and purpura - meningococcemia Signs of trauma – suspicious bruises
- 41. NEUROLOGIC EXAM Examination of the eyes, in addition to determining the presence or absence of papilledema, provides other etiological clues. Small or large pupils that respond poorly to light, or impaired eye movements suggest a drug or toxic exposure. Fixed deviation of the eyes in one lateral direction may indicate that (1)The encephalopathy has focal features (2)Seizures are a cause of the confusional state (3)Seizures are part of the encephalopathy. The general and neurological examinations should specifically include a search for evidence of trauma, needle marks on the limbs, meningismus, and cardiac disease.
- 42. Cranial Nerve Exam I. olfactory-smell II. Optic-Visual acuity, visual fields, pupils reaction, color III. Oculomotor - eye movement IV. Trochlear eye movement V. Trigeminal Nerve - facial sensation, corneals, VI. Abducens-eye movement VII. Facial nerve - motor and sensory to face VIII. Acoustic nerve - hearing IX. Glossopharyngeal - gag reflex, elevate palate X. Vagus - swallowing movement of the cords XI. Accessory Nerve - sternocleidomastoid muscle , trapezius function XII. Hypoglossal nerve - tongue movement, fasciculations
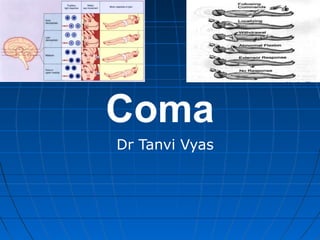
- 43. Level of lesion Level of lesion Motor response Pupillary response Respiratory Pattern Cortex Flexion withdrawal Small reactive Normal or cheyne stokes Thalamus Abn. Flexion ( decortication) Small reactive Normal or cheyne stokes Midbrain Abn. Extension (decerebration) Fixed midposition Hyperventilation Pons No response pinpoint Normal or apneustic Medulla No response Small reactive irregular
- 44. Corneal reflex Test the fifth nerve sensory and seventh nerve motor Cotton on cornea and look for a blink or watch the lower eyelashes move toward the midline Good test for mid and low pontine dysfunction
- 45. Oculocephalic Reflex DOLLs Eye Tests-sensory from the eighth nerve Motor Part of the 3rd, 4th6thnerves Can only be done in patient with stable spine Turn the head quickly to the side and the eyes should move to the opposite directions of the movement
- 46. Cold Caloric Response Oculovestiublar reflex Tests the same pathway as doll’s eyes but can be done in patient with unstable cervical cord. Elevate the head 30 degrees place a catheter in the ear and inject ice water. In an awake patient: nystagmus COWS: Cold water - fast component opposite Warm water – Same side When supratentorial disease develops Due to metabolic depression of cortical function - the fast component disappears and the eyes move toward the cold water stimulus
- 47. Respiratory Pattern Injury location and type of breathing Post hyperventilation apnea -bilateral hemispheric dysfunction or can result from bilateral damage anywhere along the descending pathway between the forebrain and upper pons Cheyne-stokes breathing (periods of hyperpnea alternate with periods of apnea) Central Neurogenic Hyperventilation (formerly known as Ondine’s curse) a sustained, rapid, deep hyperventilation ,loss of involuntary respiration
- 48. Flexion of the upper limb with extension of the lower limb (decorticate response) and extension of the upper and lower limb (decerebrate response) indicate a more severe disturbance and prognosis.
- 49. Infratentorial lesions Brainstem symptoms are often seen initially Sudden onset of coma Cranial nerve abnormalities Alteration of the respiratory pattern
- 51. Laboratory Work up CBC with diff PT,PTT, INR LFT’s Toxic screen Blood, urine culture Chest x-ray Urine ketones, glucose Electrolytes Ca, Mg, BUN, creatinine
- 52. Other Lab work Blood ammonia Lead levels Serum cortisol Skeletal survey Amino acid profile Blood pyruvate and lactate Organic acid analysis
- 53. Other test to consider EEG MRI Echocardiogram Head CT with contrast enhancement promptly to exclude the possibility of a mass lesion and herniation.
- 54. COMA Treatment
- 55. TREATMENT OF ELEVATED ICP INTUBATION Hyperventilate for a short period of time Keep head elevated Midline position to enhance venous drainage into the chest Check electrolytes Correct hyponatremia - produces brain swelling Restore low BP
- 56. Medical Intervention of increased ICP Decrease CSF Shunt fluid with external ventricultomy tube Diamox 25-100 mg/kg/day in 3 doses Reduce the size of other compartment Mannitol or 3% NaCl Mannitol –0.25 to 1.0 gm/ kg Infuse over 10 to 15 minutes Place foley May need to provide NS bolus to maintain BP
- 57. Na Cl 3% Give as 5ml/kg bolus over an hour Can be given in peripheral IV Sodium movement across the blood brain barrier is low. Therefore works similar to Mannitol
- 58. Treatment of elevated ICP Progression of treatment Mannitol, or 3% NaCl Sedation and pain medication Fever control Intubation ICP monitor and drainage of CSF Pentobarbital coma Surgery for decompression craniotomy
- 59. THANK YOU THANK YOU THANK YOU THANK YOU