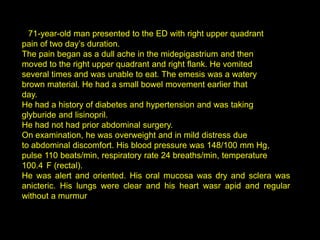
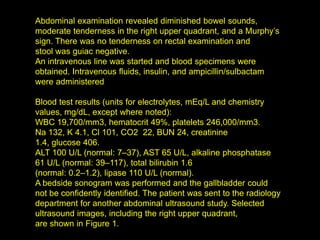
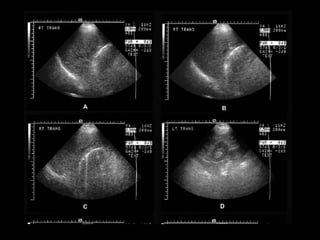
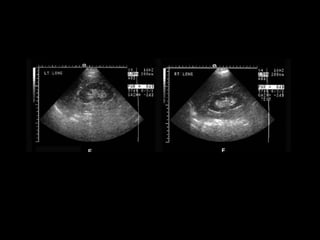
This patient presented with right upper quadrant pain that began as dull midepigastrium pain and later moved to the RUQ and flank. He vomited brown fluid and was unable to eat. Examination revealed tenderness in the RUQ and Murphy's sign. Ultrasound could not identify the gallbladder initially but was later seen on radiology ultrasound with stones. Laboratory results showed elevated WBC, glucose, ALT, AST, and lipase. The diagnosis was acute cholecystitis confirmed by ultrasound findings of gallbladder wall thickening, pericholecystic fluid, and sonographic Murphy's sign.
















































































![Hypothalamus short ppt by Dr. Neha [PT].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/hypothalamusbydr-260124145759-b9f94a93-thumbnail.jpg?width=640&height=640&fit=bounds)










