This document is the 11th edition of Clinical Anatomy: Applied anatomy for students and junior doctors by Harold Ellis. It provides a revision and applied anatomy text for clinical students. The book contains detailed information on the anatomy of the thorax, abdomen, pelvis, upper limb, lower limb, head and neck, and central nervous system. It includes sections on surface anatomy, bones and joints, muscles, blood vessels, nerves, internal organs and their applied clinical relevance.



























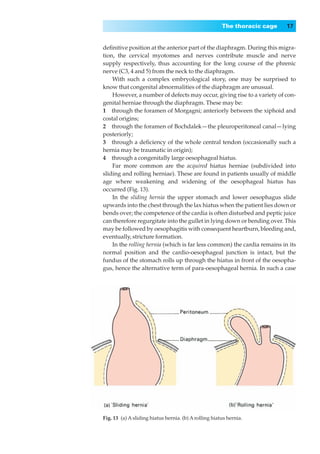


















































































































































































































































































































































































































































![Bd chaurasia's handbook of general anatomy, 4th edition[ussama maqbool]](https://cdn.slidesharecdn.com/ss_thumbnails/bdchaurasiashandbookofgeneralanatomy4theditionussamamaqbool-180228133937-thumbnail.jpg?width=640&height=640&fit=bounds)










































