Download to read offline

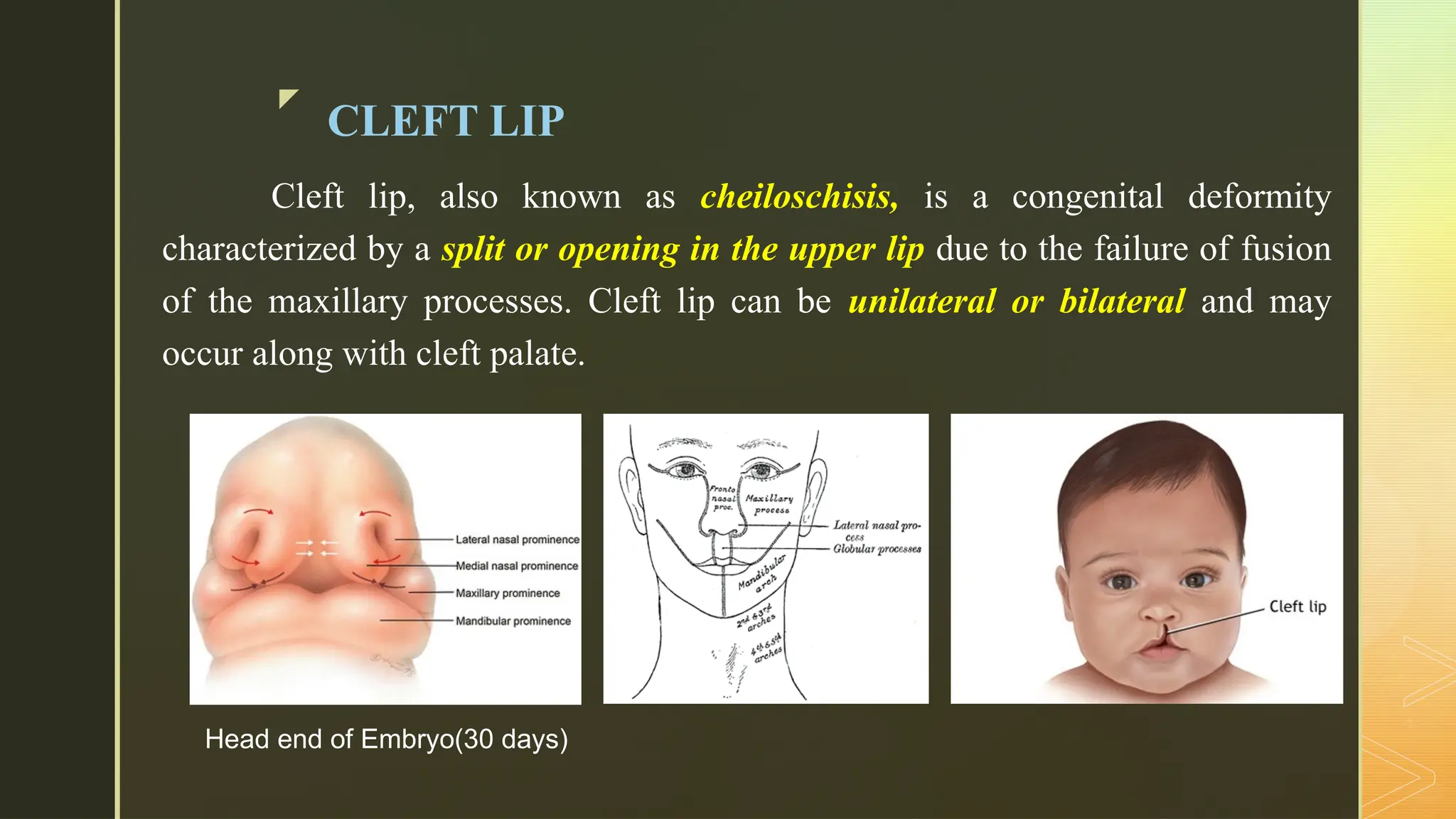


















Cleft lip, also known as cheiloschisis, is a congenital deformity characterizedbyasplitoropeningintheupperlipduetothefailureoffusion of themaxillaryprocesses.Cleft lipcanbeunilateral orbilateral andmay occuralongwithcleftpalate. Head end of Embryo(30 days) z Cleft palate, also known as palatoschisis, is a congenital condition characterizedbyanopeningintheroofof themouthcausedbythefailureof fusionof thepalatineprocesses.Thisconditioncan involve thehardpalate, softpalate,orboth. z Cleft Lip: The incidence of cleft lip, withorwithout cleft palate, is approximately1 in1,000 livebirths. It ismorecommon inmales than females. CleftPalate:Theincidenceofcleftpalatealoneisabout1in2,500live births.Thisconditionismorecommoninfemalesthanmales. z Genetic Factors: Family history of clefts can increase the risk. Mutationsin geneslinked to facial development. Chromosomal abnormalities associated with conditions like trisomy 13 and Van der Woude syndrome. Theexactcauseofcleftlipandcleftpalateisunknown;however,theyare believedduetoacombinationofgeneticandenvironmentalfactors. EnvironmentalFactors: Maternal health issues such as diabetes and obesitycontribute. Nutritional deficiencies, especially folic acid, duringpregnancy. Substanceuse, including alcohol and tobacco, bythemotherduringpregnancy. Exposure to X-rays or radiation during pregnancy. Overuse of certain medications like anticonvulsantsduringpregnancy. z Cleft lip and cleft palate result from abnormal fusion of facial structures during embryonic development. The lip forms from the merging of the medial nasal processes and maxillary processes, while the palate develops from the fusion of palatine shelves. Disruptions in these processes can lead to incomplete formation, resulting in gaps. These malformations can lead to problems such as difficulty eating, speech delays, ear infections, and orthodontic issues. z FeedingDifficulties: Infantsmaystruggletocreateaproperseal forbreastfeedingorbottle feeding,leadingtoinadequatenutrition. SpeechDelays:Cleftscanaffectthedevelopmentofnormalspeechpatterns,requiringspeech therapy. EarInfections:IncreasedriskofotitismediaduetoEustachiantubedysfunction,whichcan leadtohearingloss. RespiratoryInfections:Higher susceptibility torespiratoryinfectionsdue tocompromised airwayfunction. DentalProblems:Misalignmentofteeth,missingteeth,andincreasedriskofcavities. GrowthandDevelopmentIssues:Potential impactonoverallgrowthif feedingdifficulties aresignificant. z Prenatal Ultrasound: Can identify physical abnormalities, such as cleft lip/palate, as early as the second trimester. Physical Examination: A thorough examination at birth can confirm the presence of cleft lip/ palate. z After birth, infants with cleft lip and/or cleft palate require caref



















































































