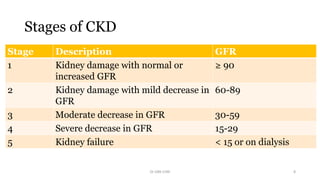
A 4-year-old boy presented with polyuria, polydipsia for 4 months and failure to thrive for 3 months. He also had irregular fever for 2 months. On examination, he was pale, hypertensive, and growth retarded. Chronic kidney disease can reduce lifespan and quality of life by clogging the kidneys. It is defined as kidney damage or decreased GFR for 3 or more months. Risk factors include VUR, obstructive uropathy, previous nephritis, family history, and low birth weight. Stages range from kidney damage with normal GFR to kidney failure. Management focuses on monitoring, controlling hypertension and nutrition, and slowing progression.













































































![CASE_PRESENTATION_ON_subdural_hematoma(SDH)[1 FINAL PPT]-1.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/casepresentationonsubduralhematomasdh1finalppt-1-260129172522-d405d375-thumbnail.jpg?width=640&height=640&fit=bounds)





