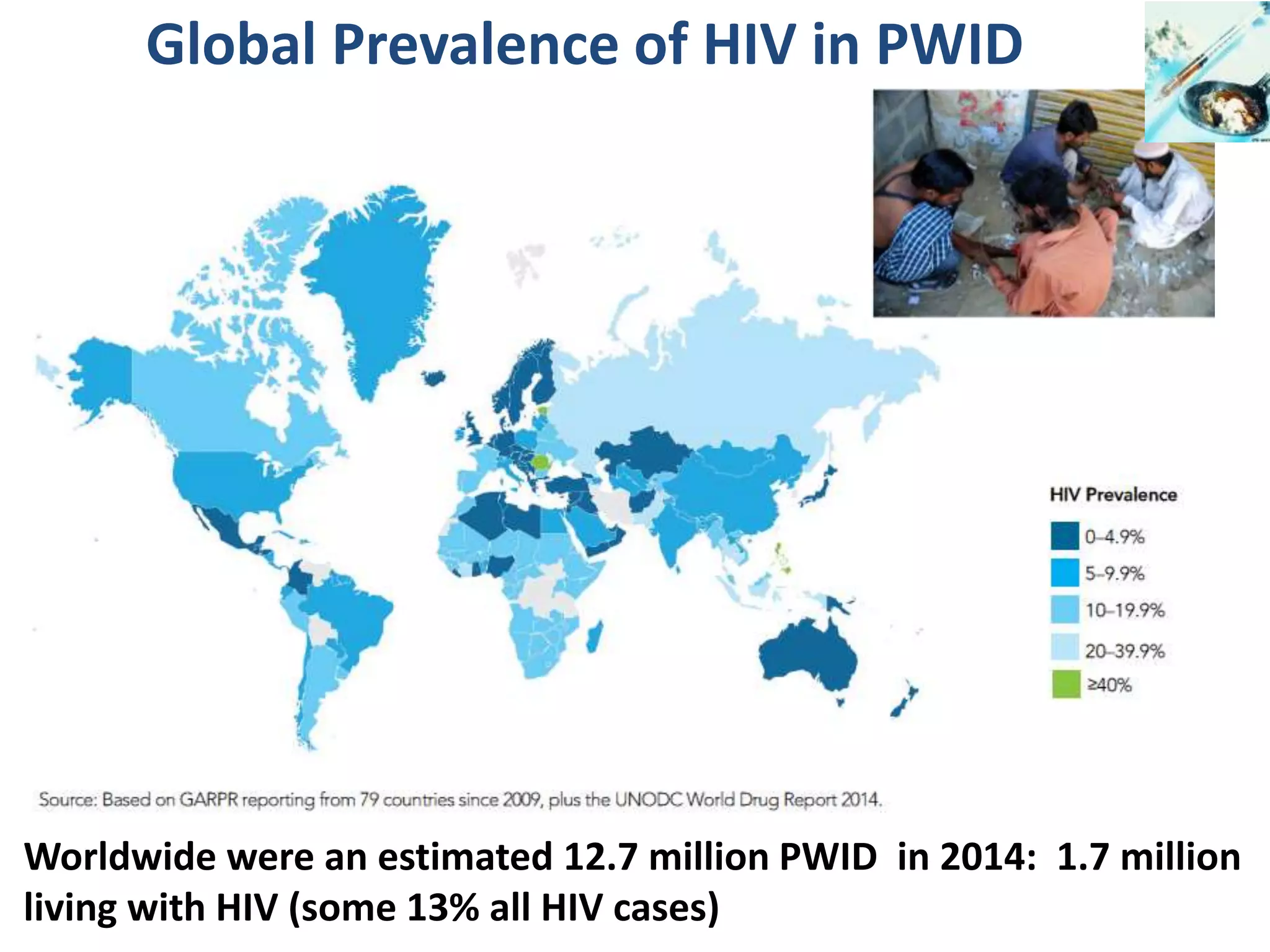
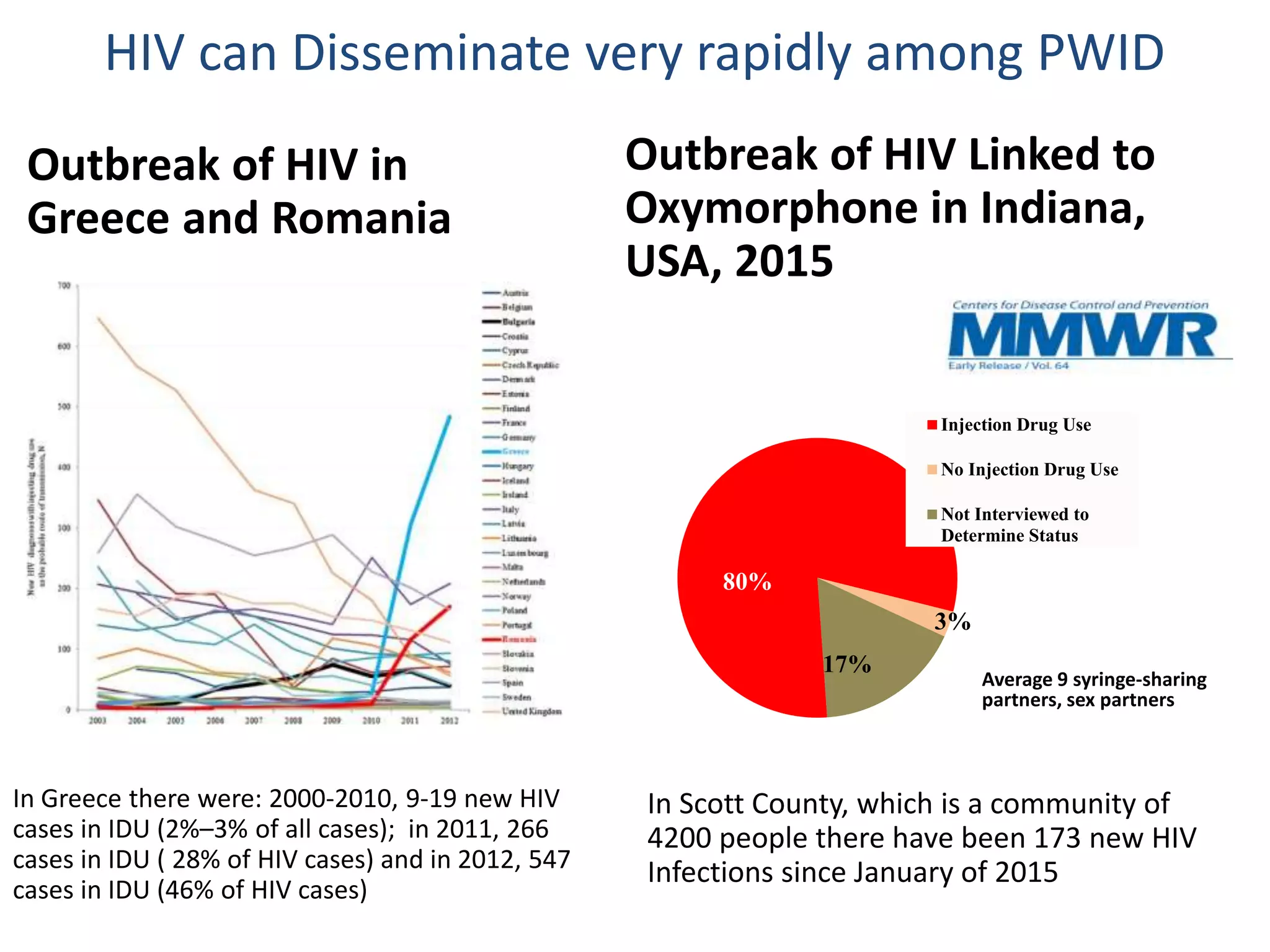
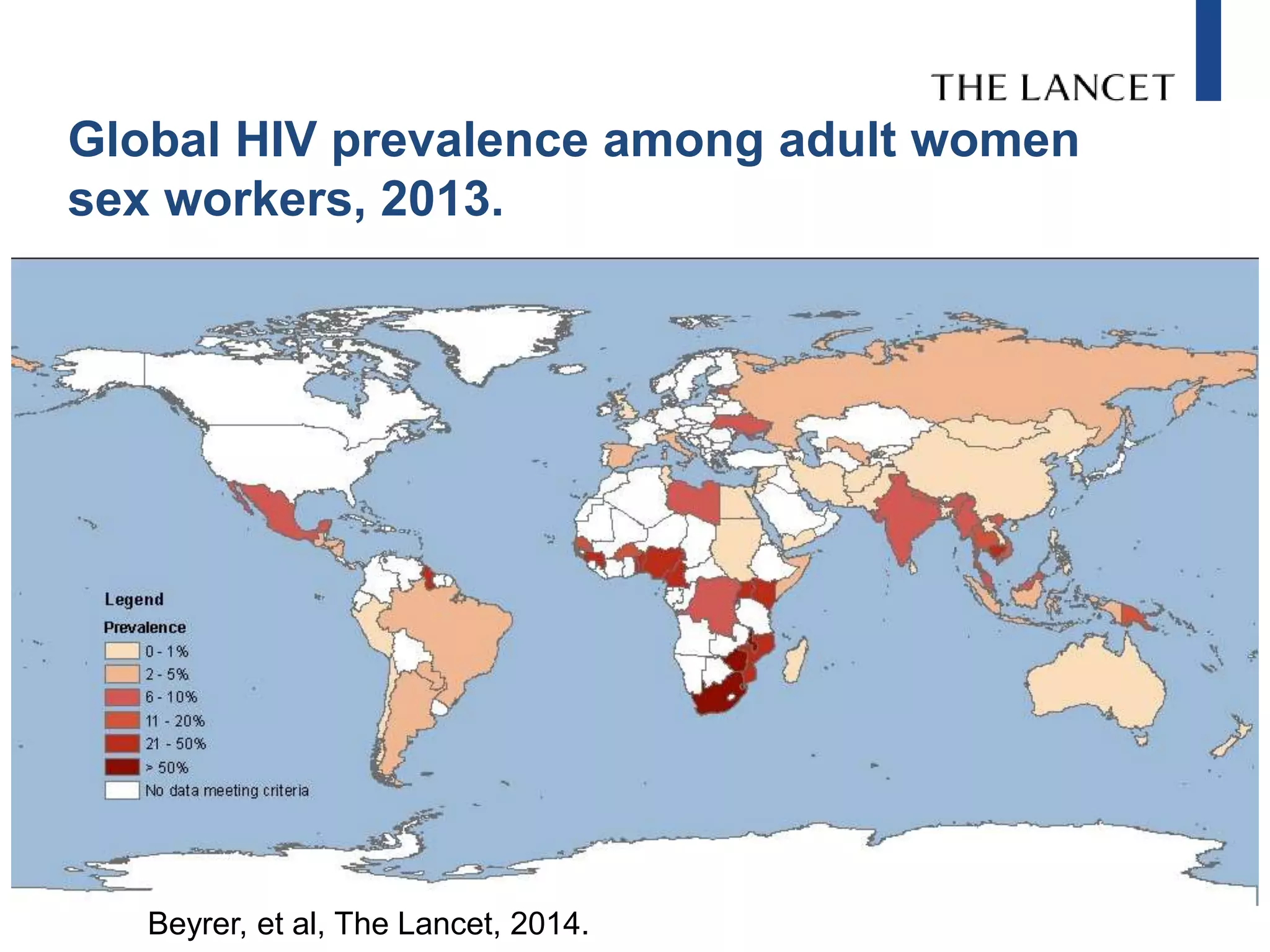
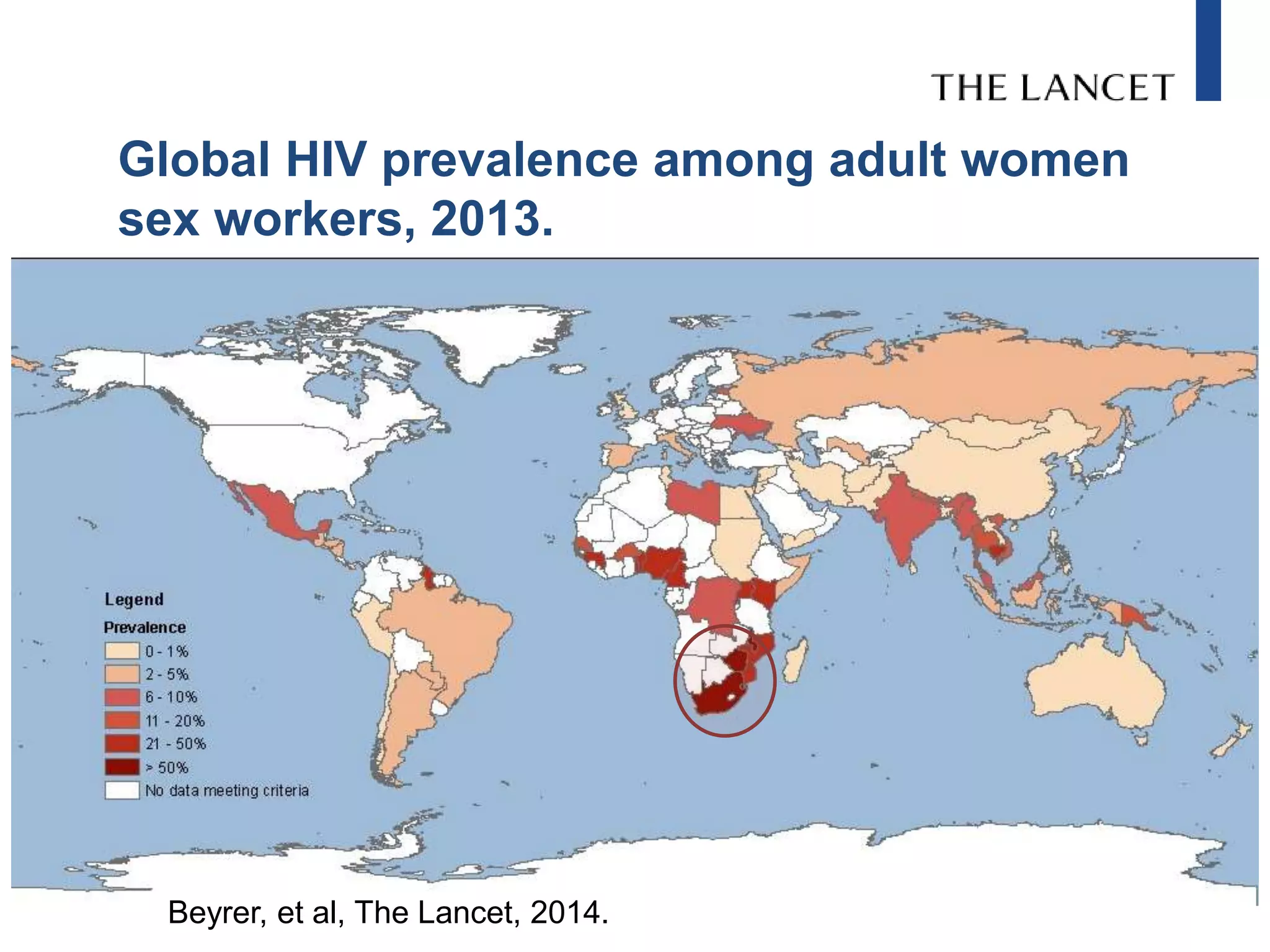
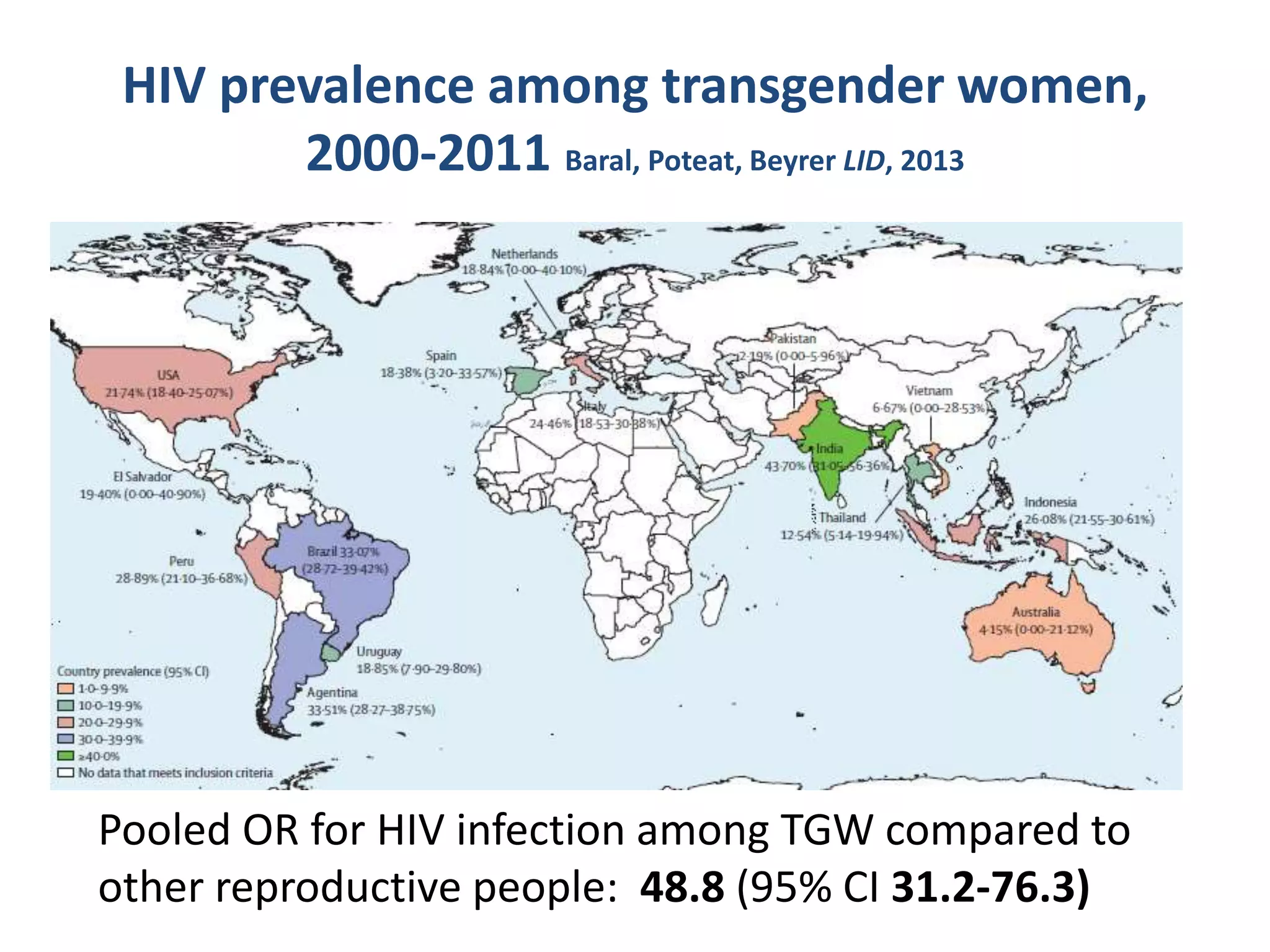
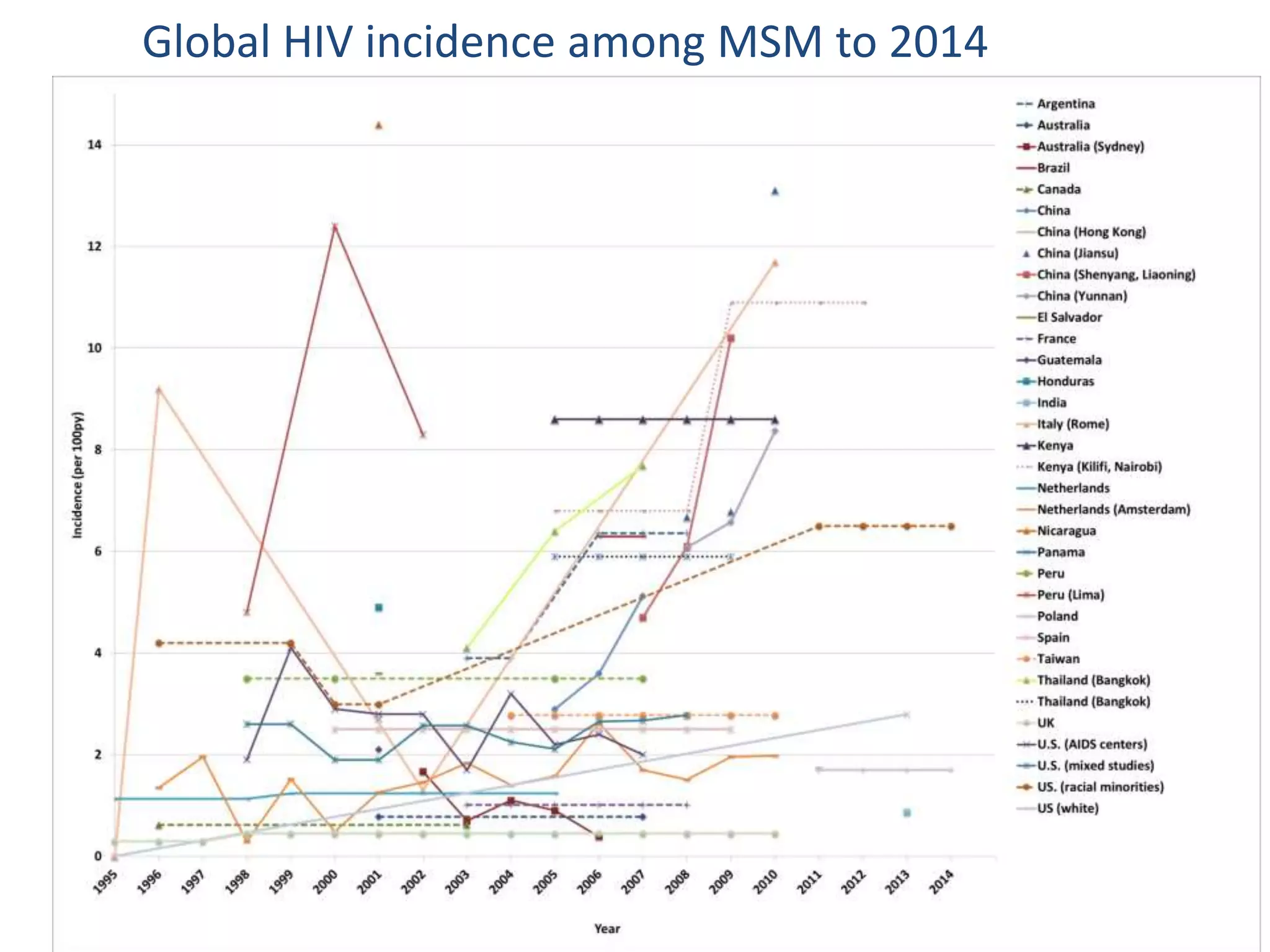
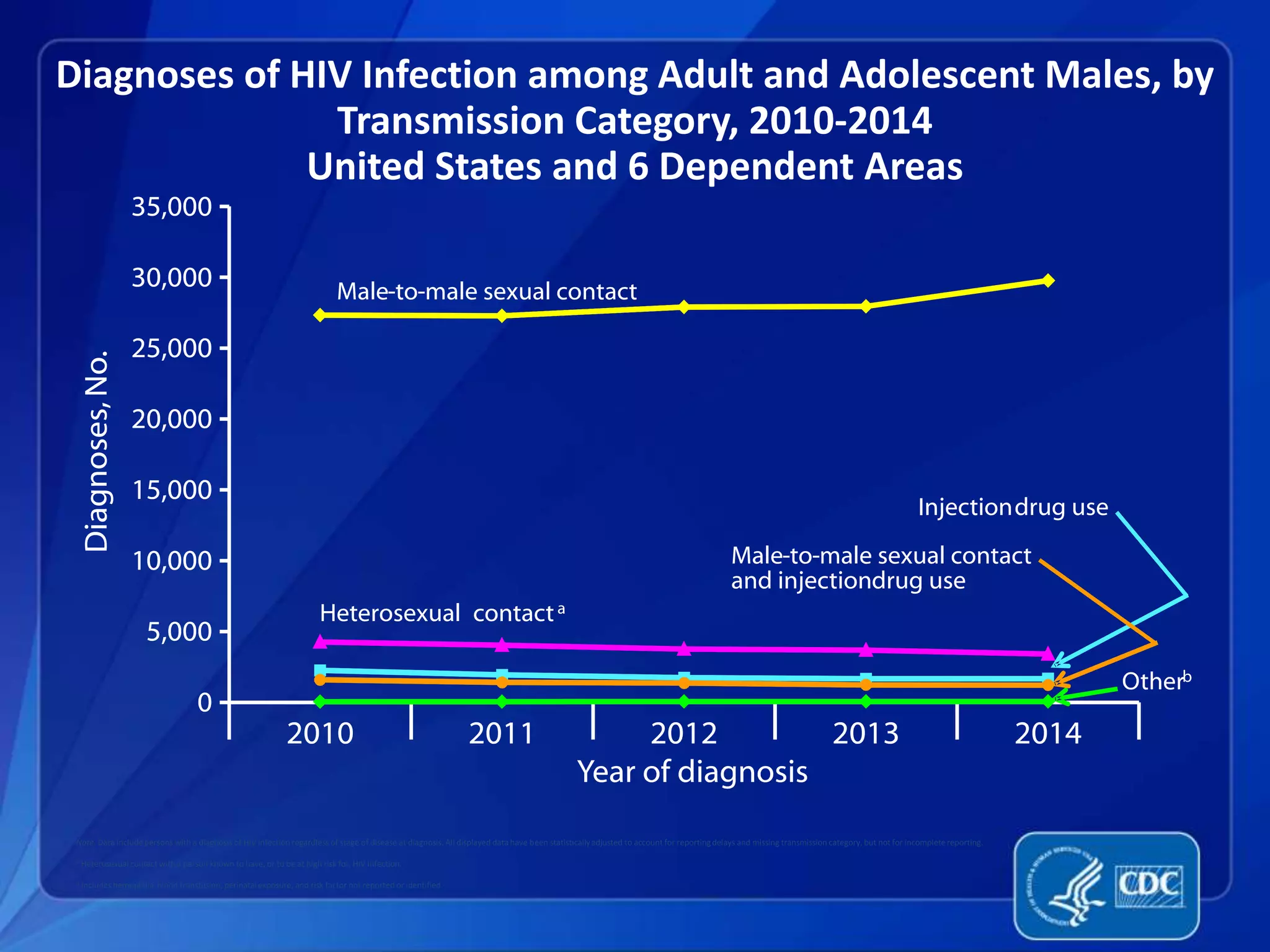
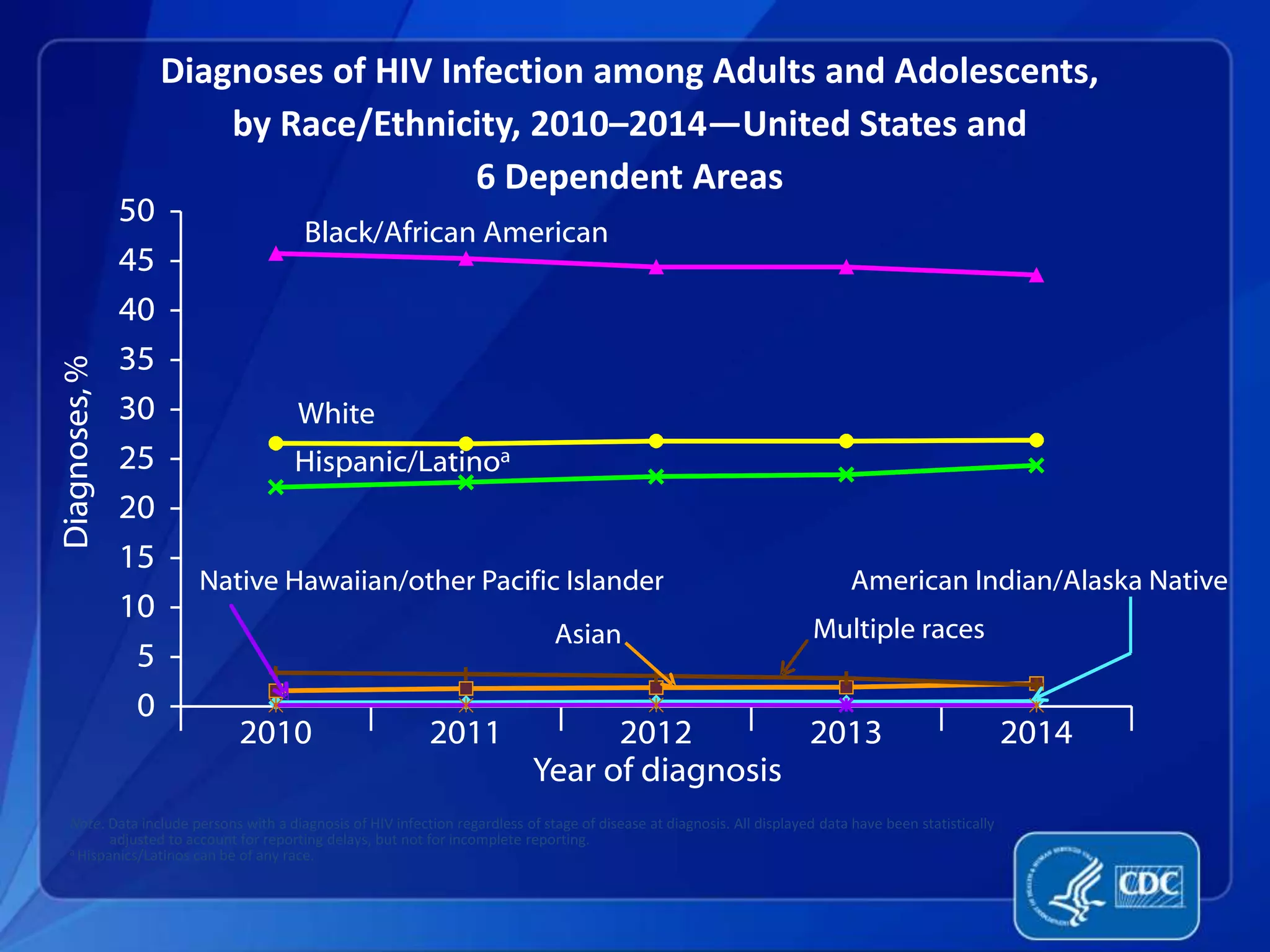
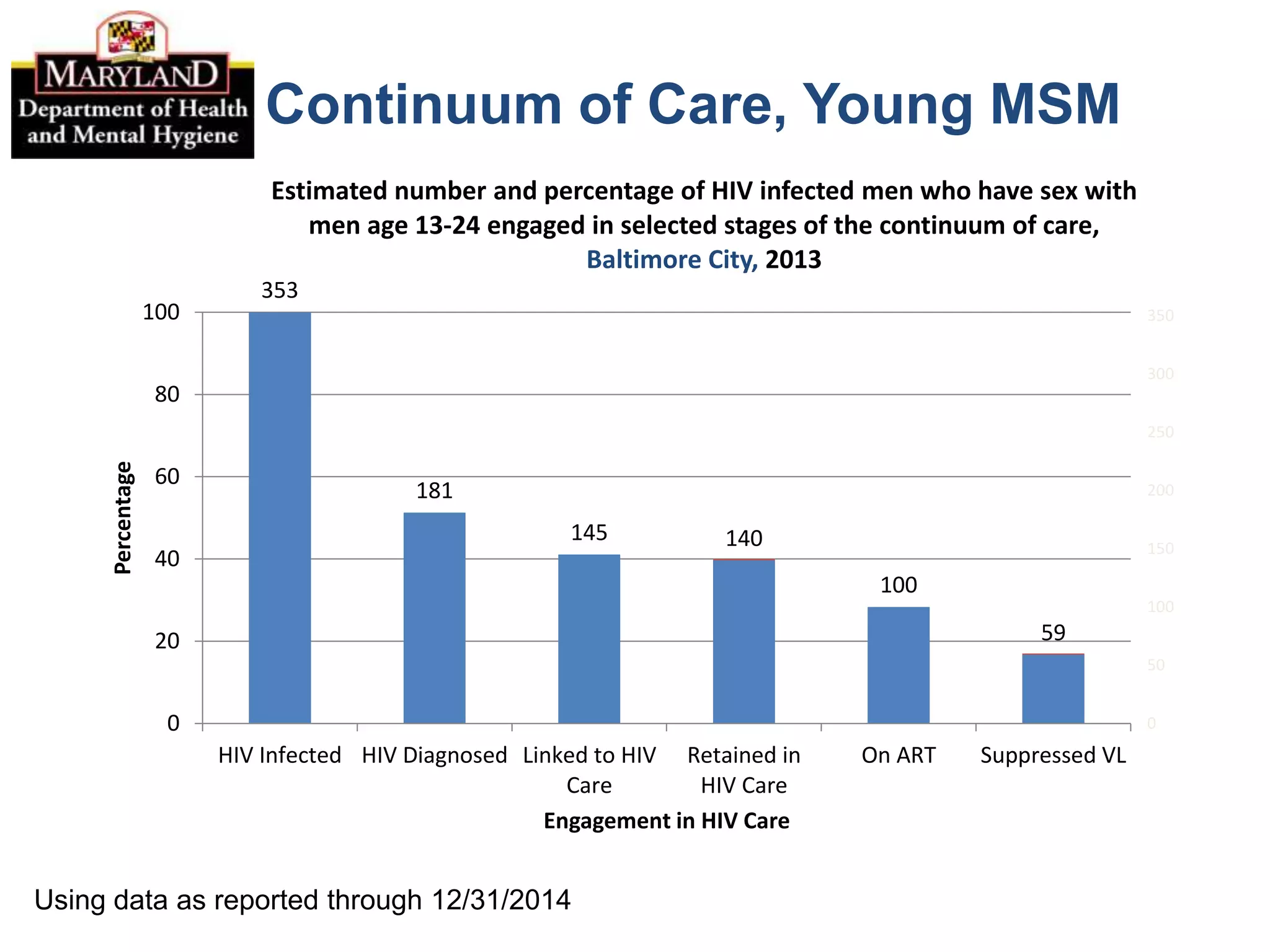
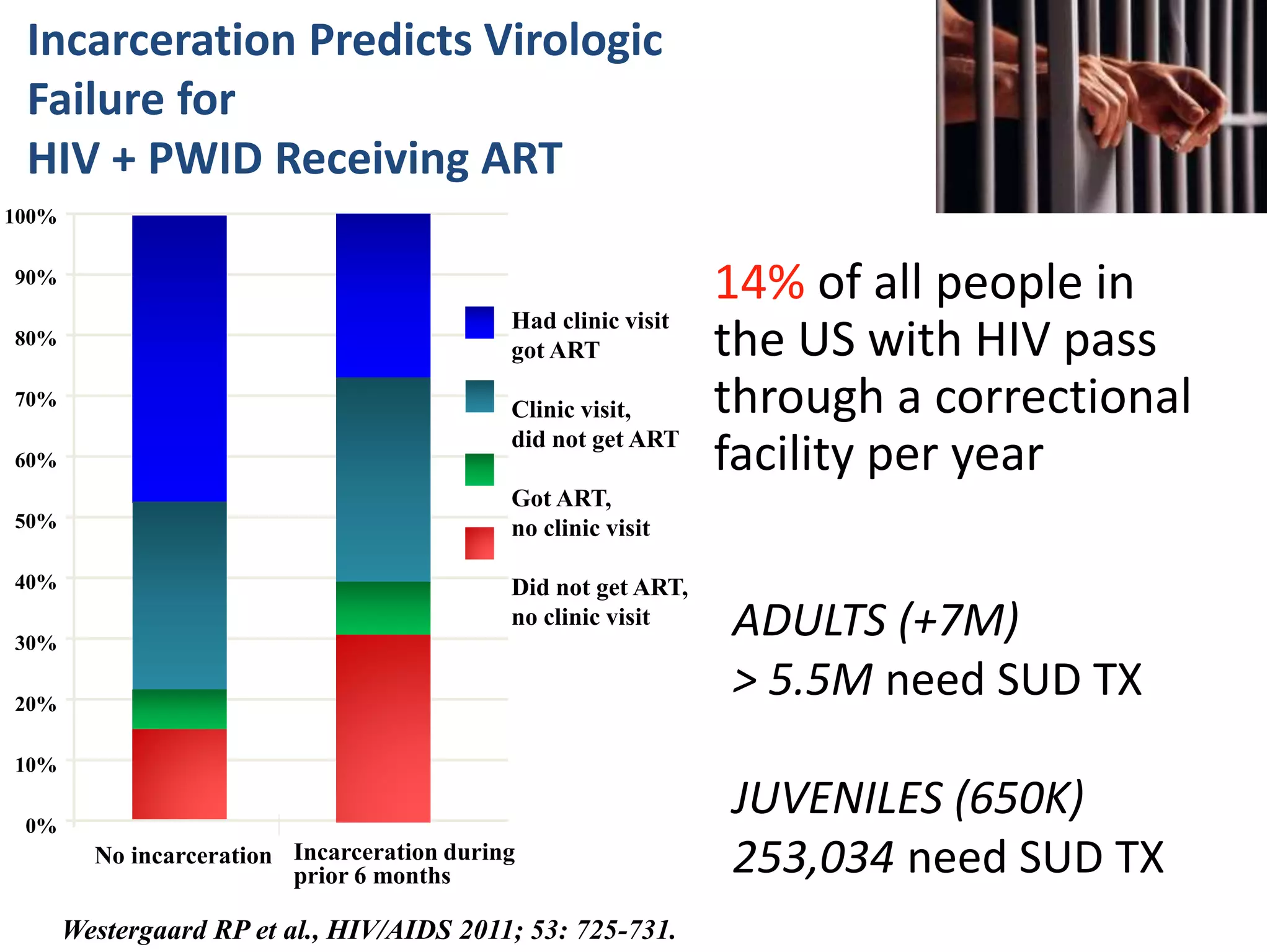
The International AIDS Society (IAS) is the world's largest association of HIV professionals, advocating for urgent action to reduce HIV's global impact and urging membership. It highlights the risks faced by key populations, including men who have sex with men, sex workers, and people who inject drugs, emphasizing the need for improved access to essential HIV services. The document discusses recent data and challenges in HIV prevention and treatment, as well as legislative impacts on these populations, particularly in Nigeria.