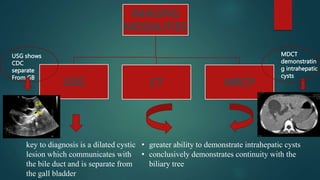
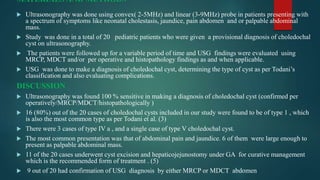
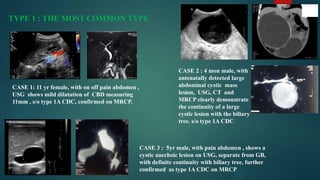
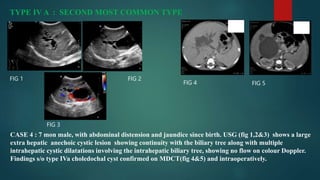
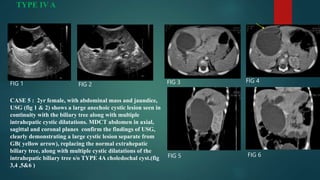
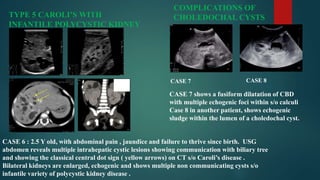
This document discusses the evaluation of choledochal cysts using ultrasonography in pediatric patients. It presents 6 case studies demonstrating the use of ultrasonography to diagnose different types of choledochal cysts according to the Todani classification system. Ultrasonography was found to be 100% sensitive in diagnosing choledochal cysts and identifying the cyst type in 20 pediatric patients. It can also be used to detect complications and guide management such as surgical excision.





































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)















![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)