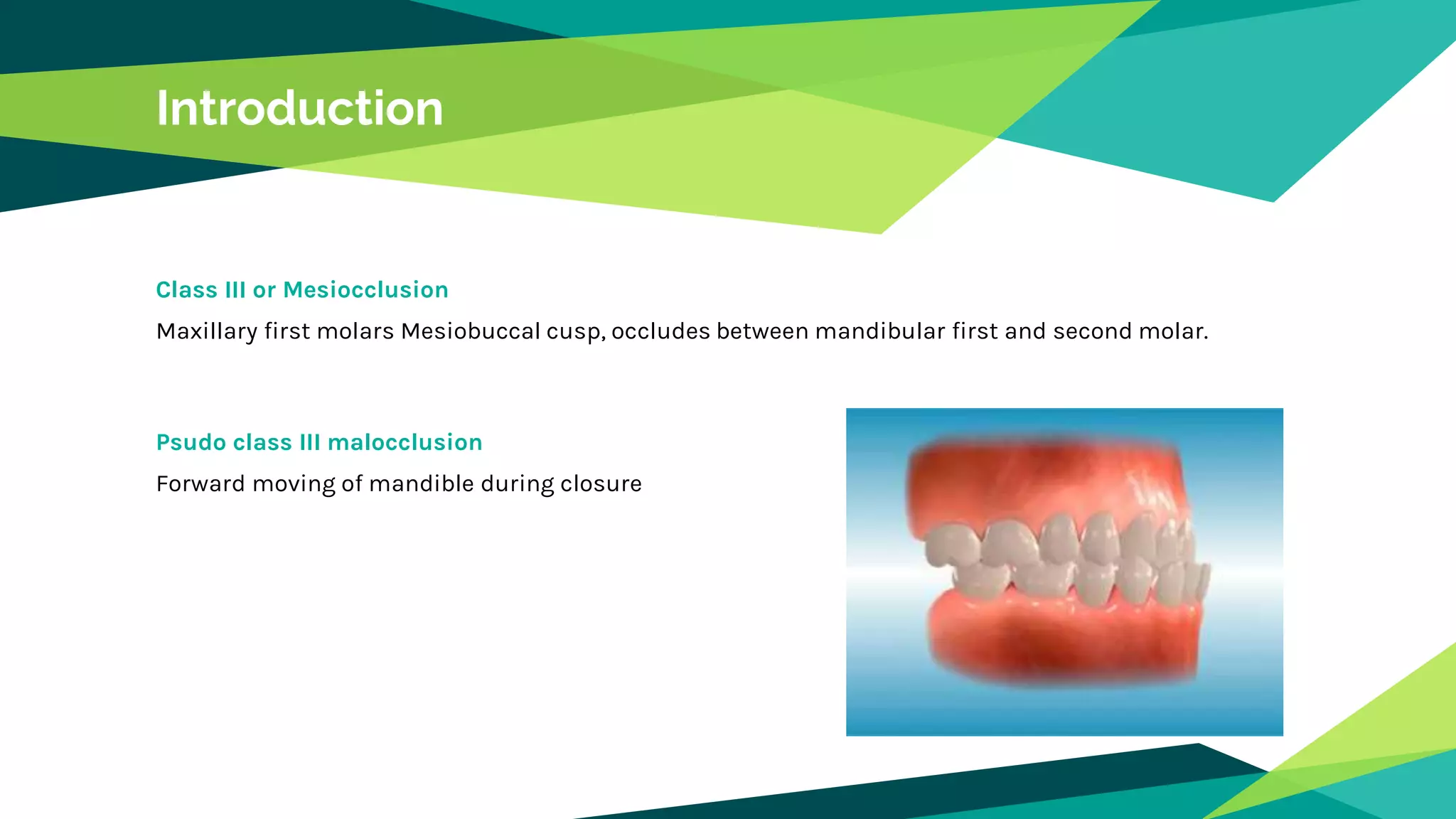
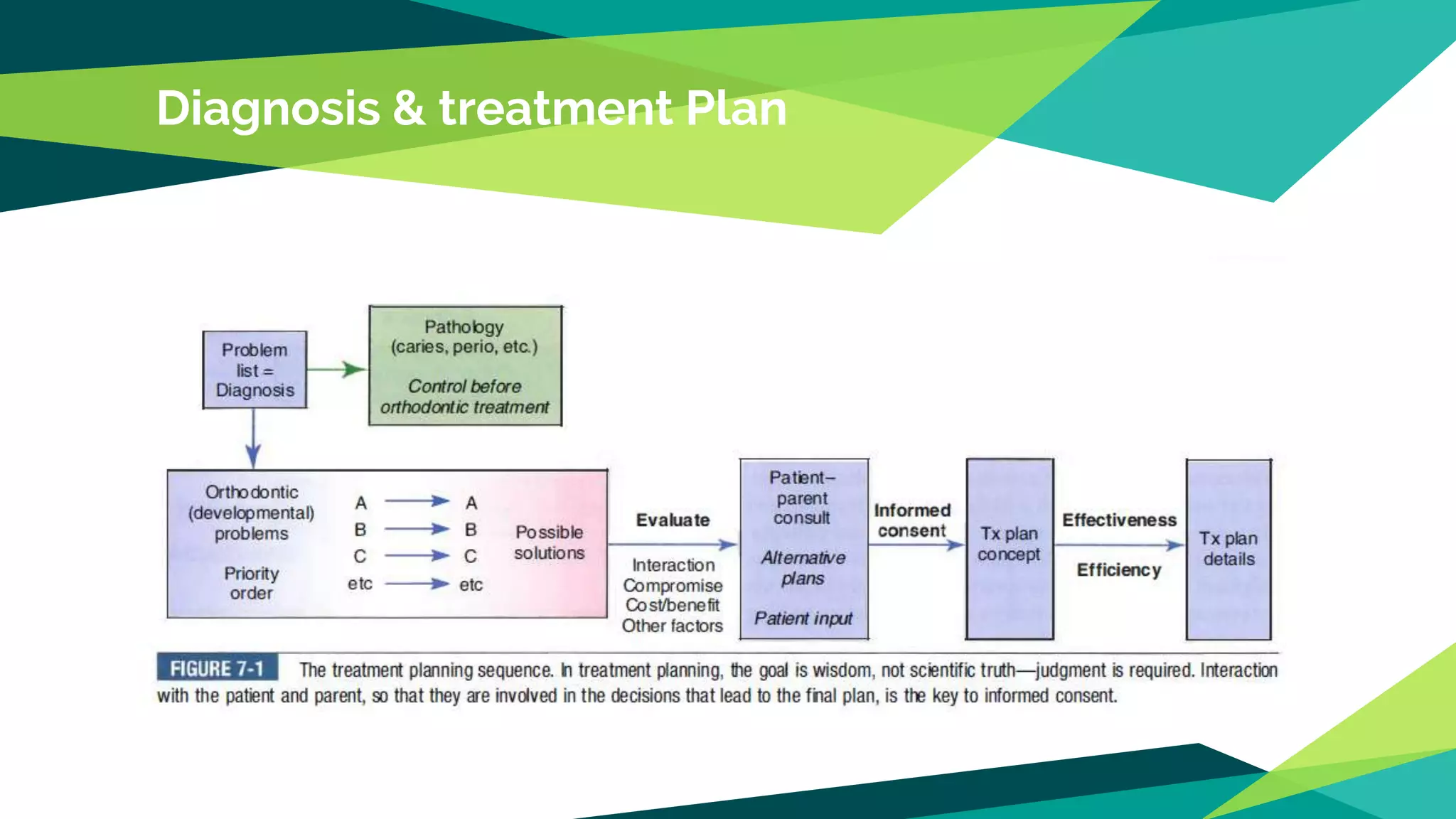
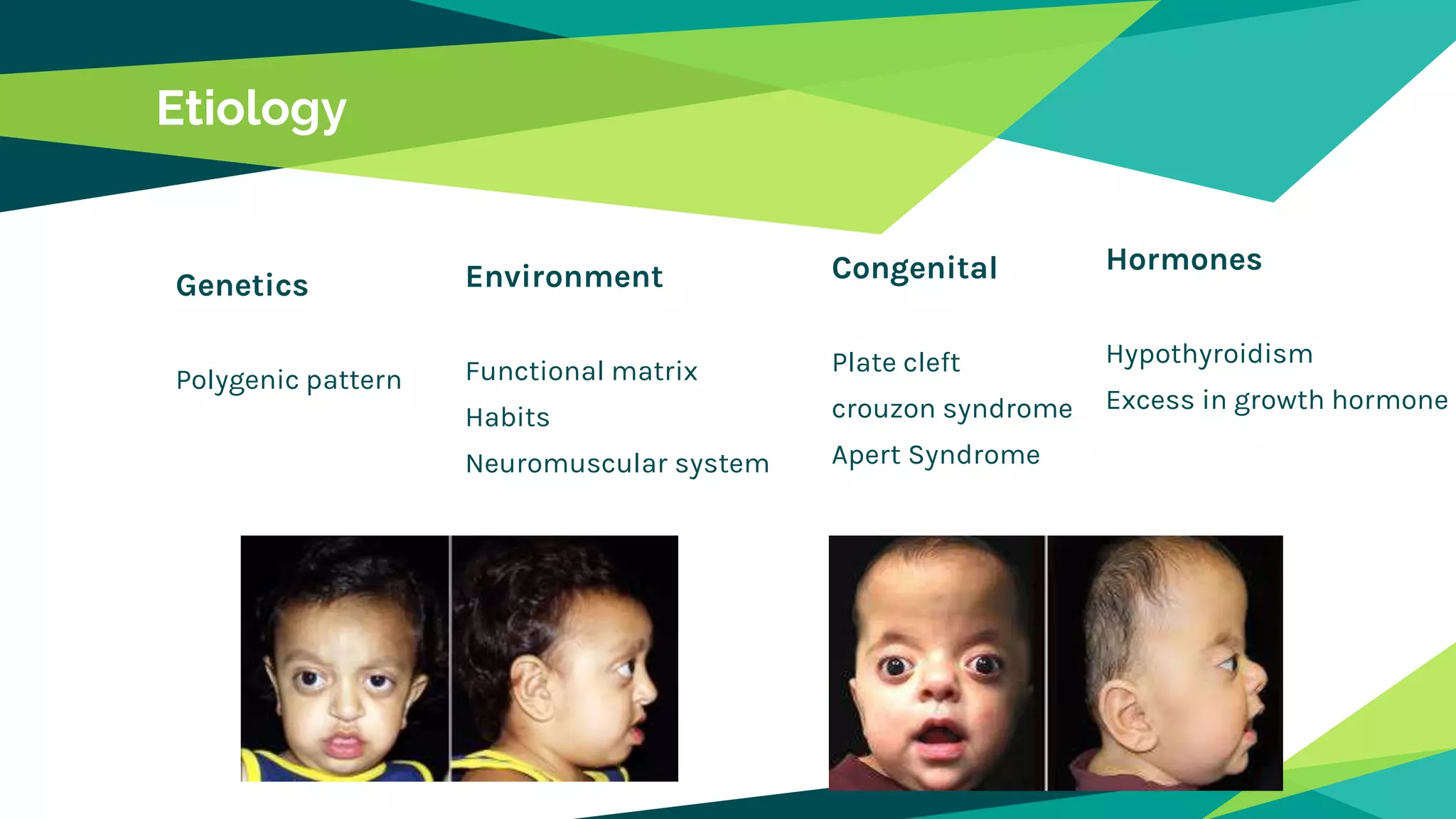
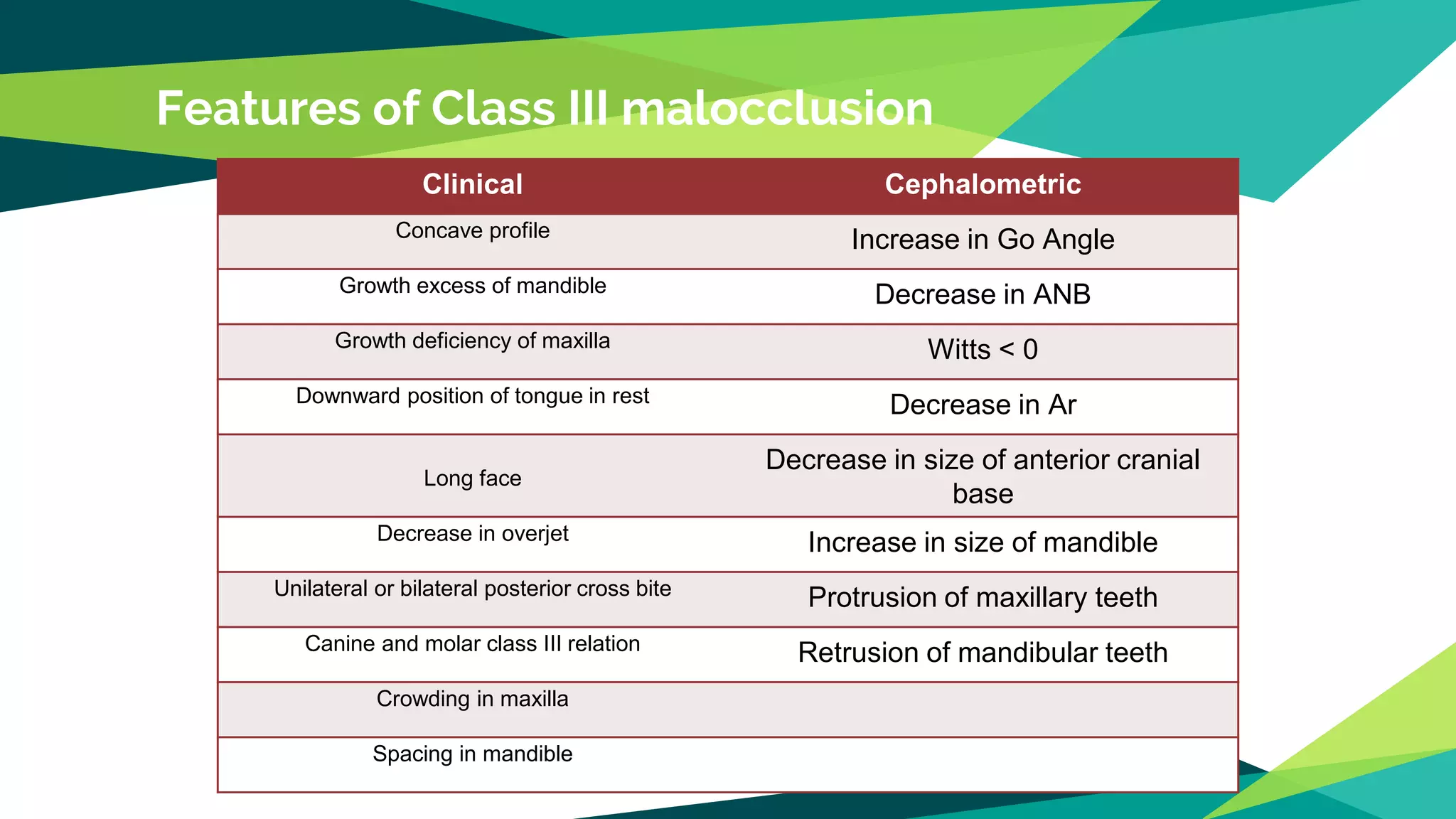
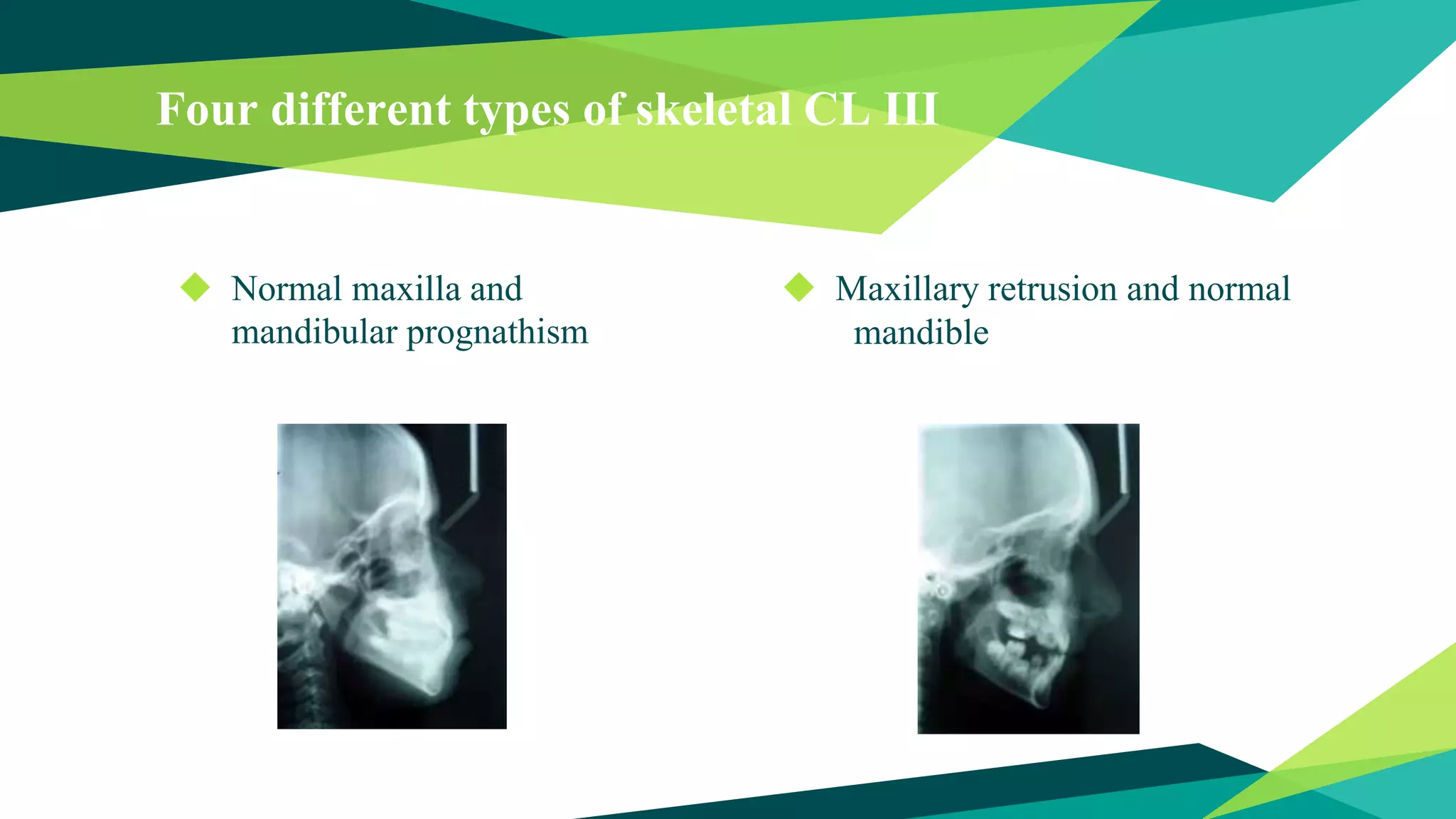
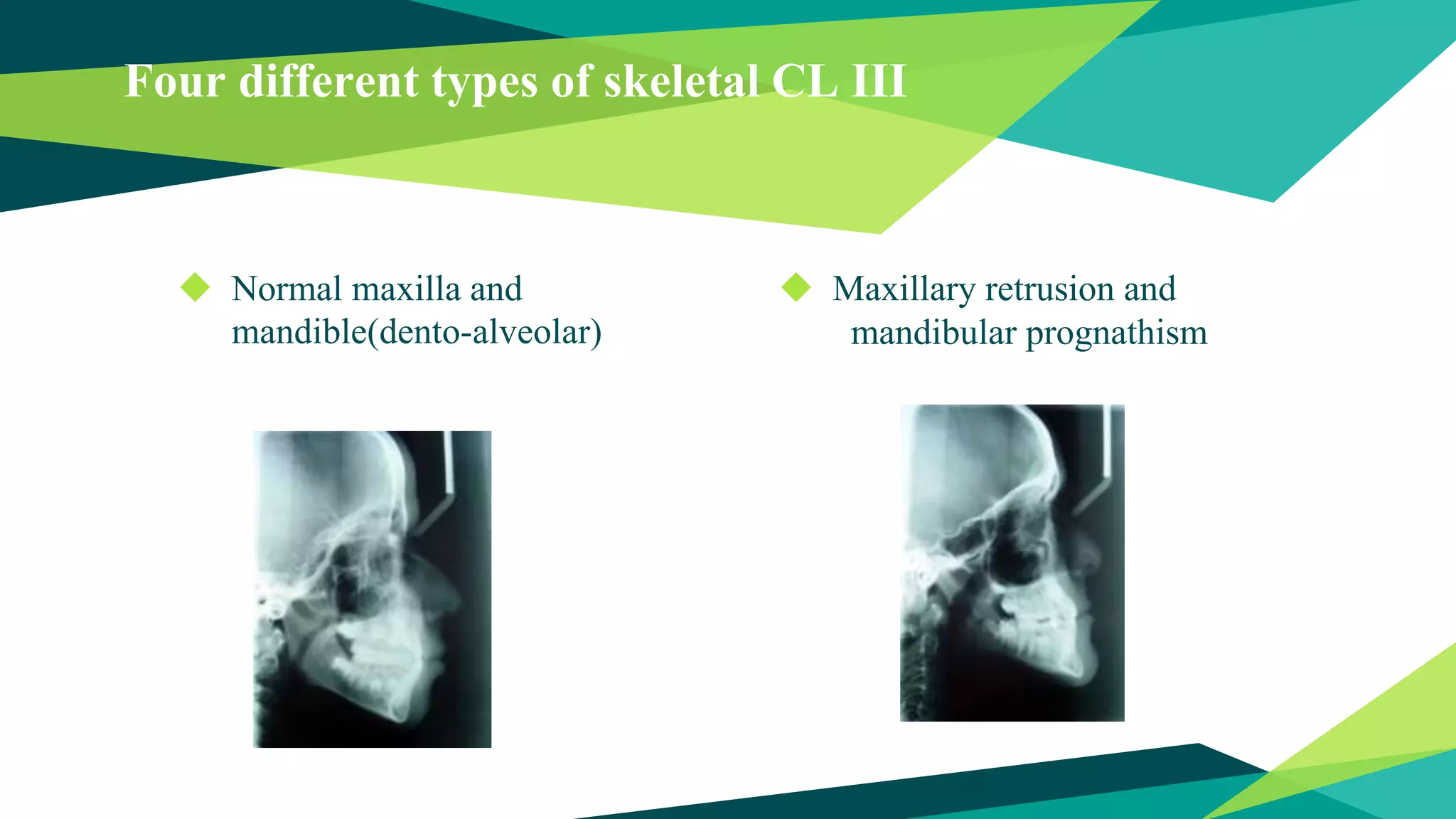
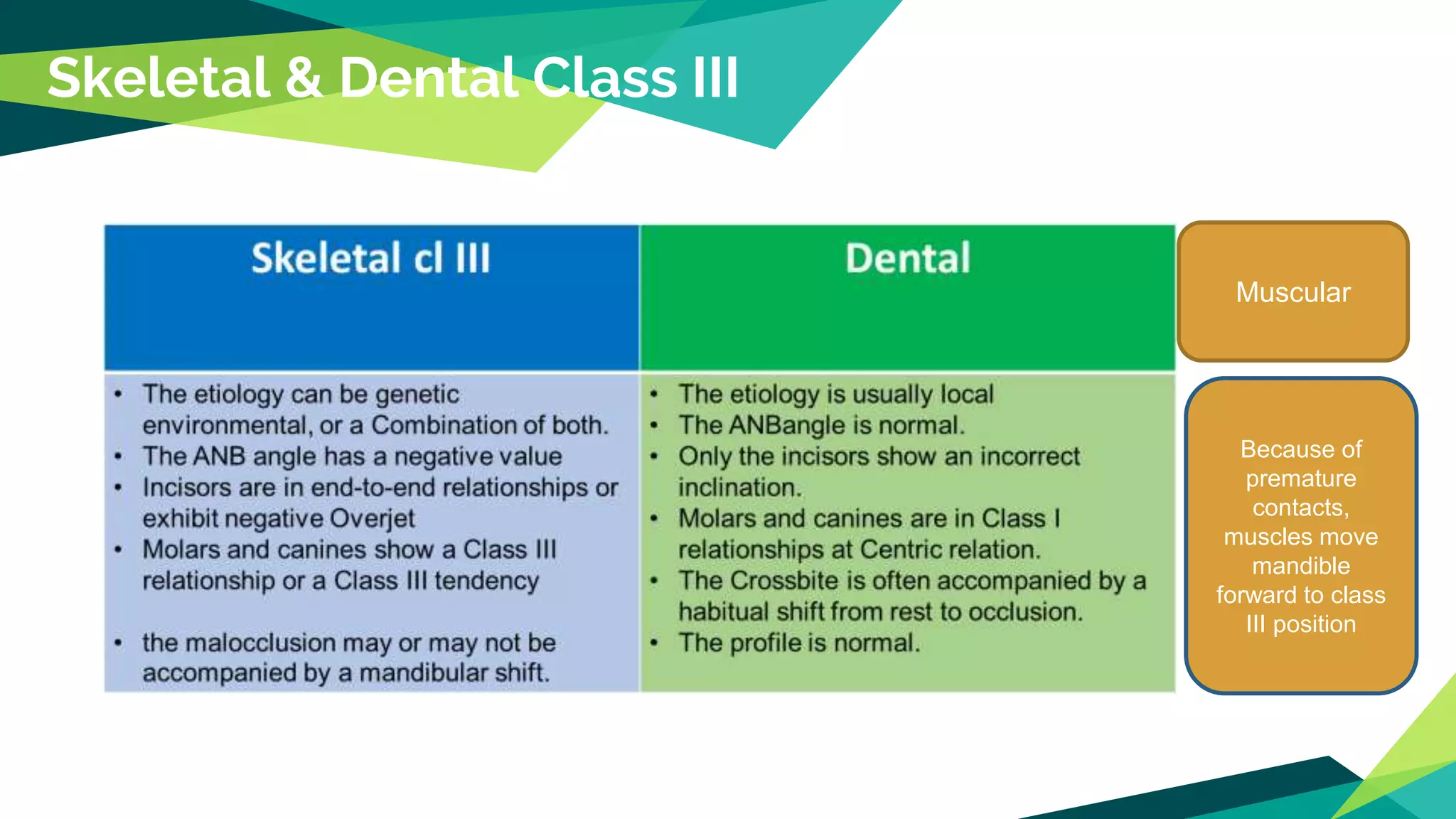
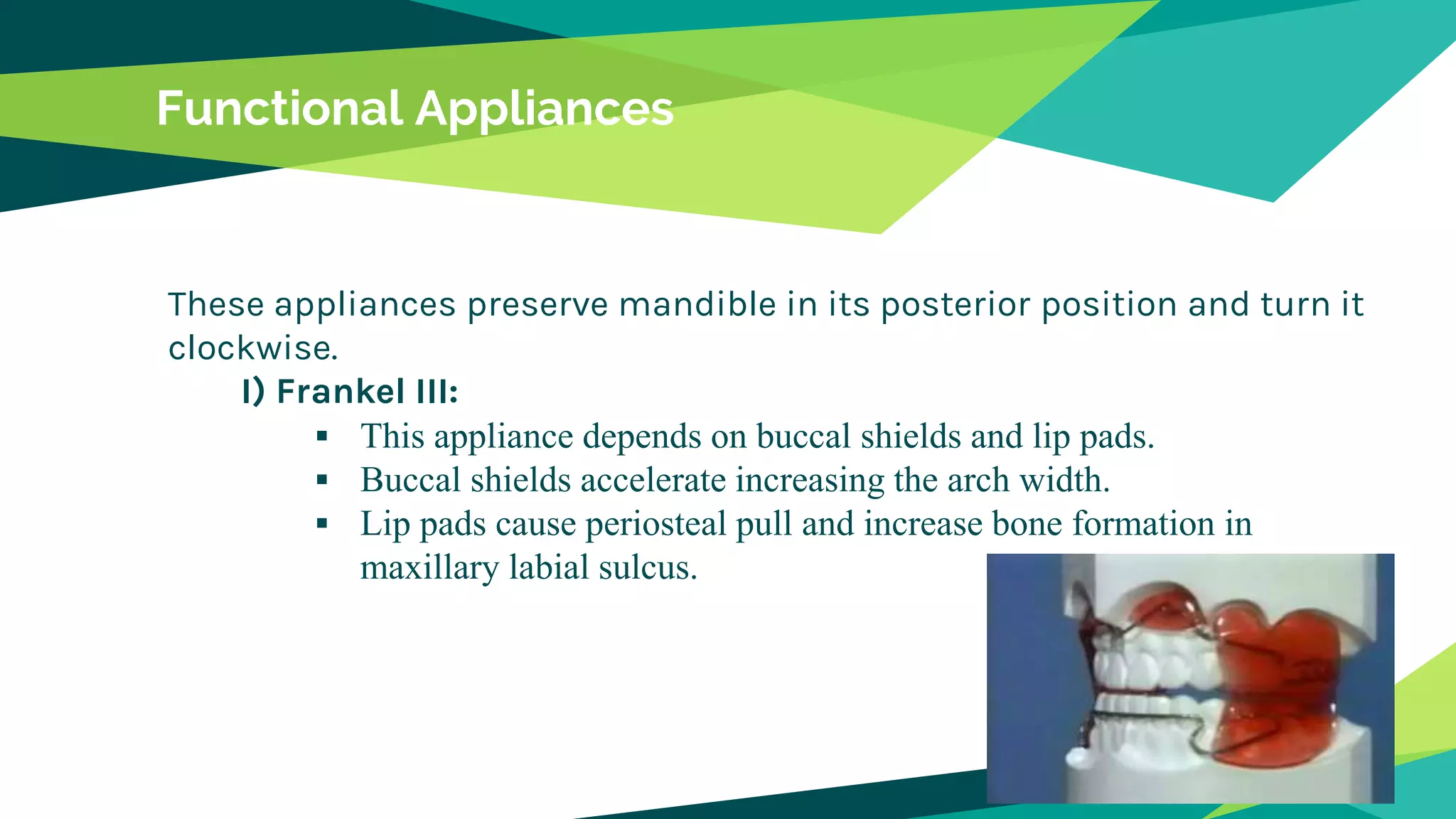
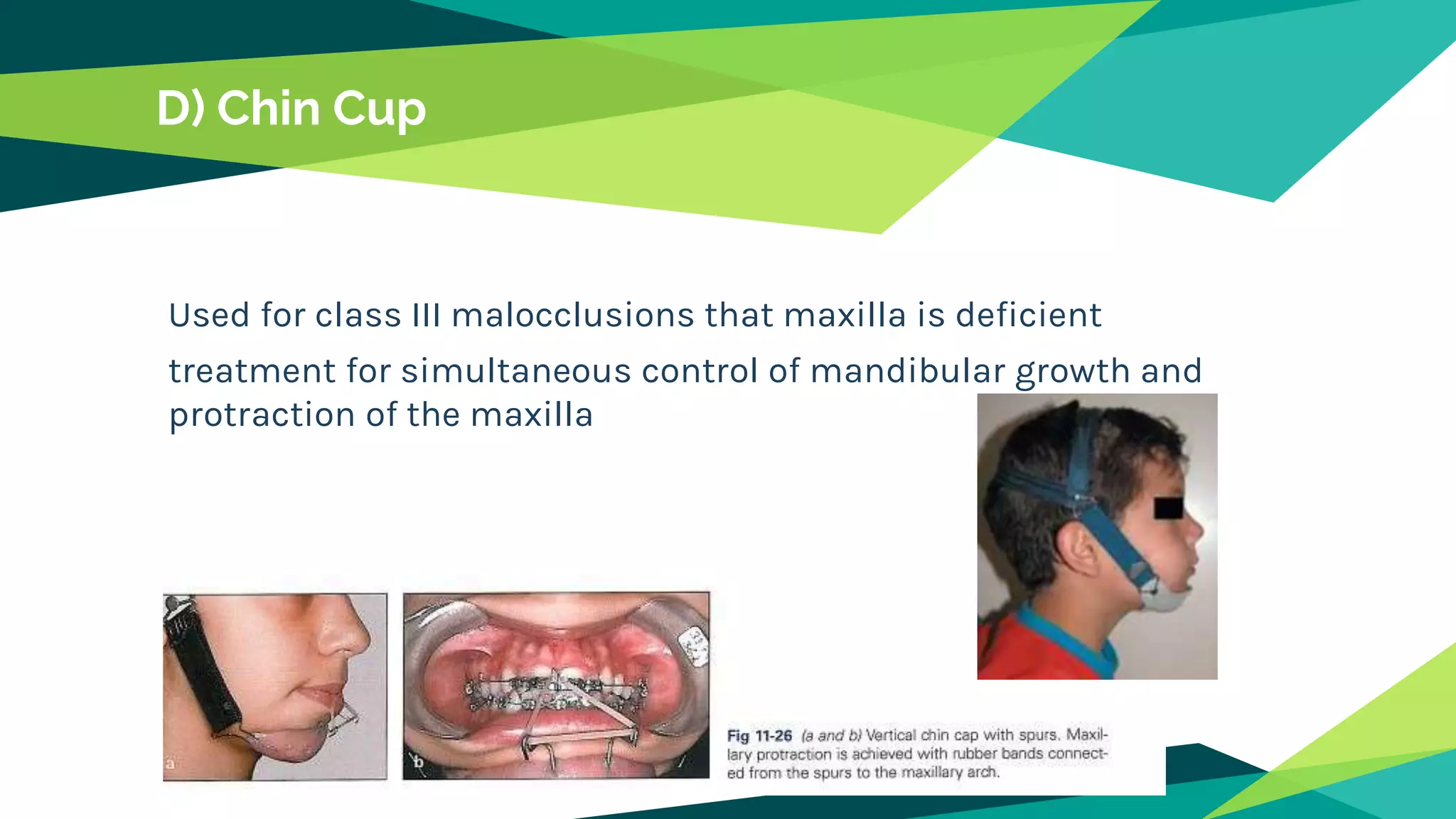
Class III malocclusion occurs when the mandible is positioned forward in relation to the maxilla. It can be caused by maxillary deficiency, mandibular excess, or a combination. Diagnosis involves measuring angles like ANB and Wits appraisal. Treatment depends on the underlying skeletal discrepancy and may involve functional appliances to guide growth, facemasks to protract the maxilla, or chin cups to restrain mandibular growth. For older patients, camouflage options like extractions and orthodontic tooth movement are used. Early treatment is preferred to prevent adverse effects on facial growth and development.
























































![Apporach to lung biopsy [Auto-saved].pptx latest](https://cdn.slidesharecdn.com/ss_thumbnails/apporachtolungbiopsyauto-saved-251211225655-93258539-thumbnail.jpg?width=640&height=640&fit=bounds)











