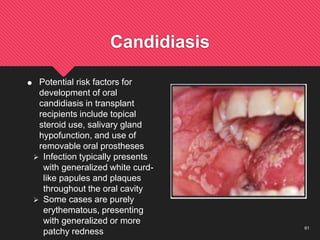
Organ transplantation can restore organ function for patients with certain medical conditions. It is sometimes the only life-saving option. Key factors in transplantation include proper donor-recipient matching, immunosuppressive therapy to prevent rejection, and limiting risks from long-term immunosuppression like infection. Major transplant organs include kidney, heart, liver, lungs, and pancreas. Outcomes have improved due to advances in matching, immunosuppression, and surgery.