Downloaded 105 times
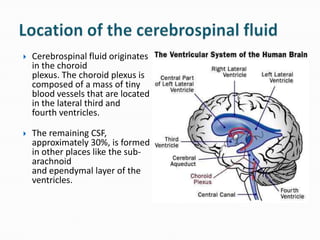



1. Gustavo Duarte Viana is a student at Kursk State Medical University who wrote a document about cerebrospinal fluid in 2012 as part of a group project. 2. The document discusses the anatomy, formation, circulation, functions, and clinical analysis of cerebrospinal fluid. It describes how CSF is produced in the ventricles of the brain and circulates around the central nervous system to perform important protective and nutrient functions. 3. The document provides details on how CSF is sampled and analyzed, including normal ranges for various chemical components and abnormalities that can be observed. It also briefly discusses meningitis and Dandy-Walker syndrome as conditions related to CSF.




























































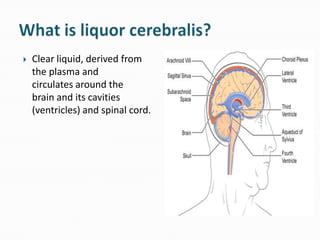
![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)














