(👑VVIP ISHAAN ) Russian Call Girls Service Navi Mumbai🖕9920874524🖕Independent...
Mahmoud
1. Central venous catheter
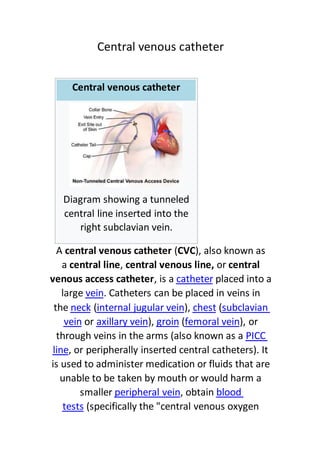
Central venous catheter
Diagram showing a tunneled
central line inserted into the
right subclavian vein.
A central venous catheter (CVC), also known as
a central line, central venous line, or central
placed into acathetera, isvenous access catheter
. Catheters can be placed in veins inveinlarge
subclavian(chest),internal jugular vein(neckthe
), orfemoral vein(groin),axillary veinorvein
PICCthrough veins in the arms (also known as a
, or peripherally inserted central catheters). Itline
is used to administer medication or fluids that are
unable to be taken by mouth or would harm a
blood, obtainperipheral veinsmaller
(specifically the "central venous oxygentests
2. central venoussaturation"), and measure
[2][1]
.pressure
]editMedical uses[
Central line equipment, in order of typical usage:
1.local anestheticSyringe with
2.is neededvenous cutdownScalpel in case
3.guidanceultrasoundSterile gel for
4.) on syringeGaIntroducer needle (here 18
to detect backflow of blood uponsalinewith
vein penetration
5.Guide wire
6.Tissue dilator
7.)Gadwelling catheter (here 16In
8.Additional fasteners, and corresponding
surgical thread
9.Dressing
3. lumen catheter inserted on the-twodialysisA
person's left side. Scars at the base of the neck
jugularindicate the insertion point into the left
.vein
Reasons for the use of central lines include:
antibioticsintravenousterm-Long
, especially inparenteral nutritionterm-Long
chronically ill persons
Long-term pain medications
Chemotherapy
inphlebitisDrugs that are prone to cause
peripheral veins (caustic), such as:
4. chlorideCalcium
erapyChemoth
Hypertonic saline
(KCl)Potassium chloride
Amiodarone
Vasopressors (for
)dopamine,epinephrineexample,
Plasmapheresis
Peripheral blood stem cell collections
Dialysis
Frequent blood draws
Frequent or persistent requirement for
intravenous access
peripheralNeed for intravenous therapy when
is impossiblevenous access
Blood
Medication
Rehydration
scentral venouMonitoring of the
(CVP) in acutely ill people to quantifypressure
[1]
fluid balance
5. Central venous catheters usually remain in place
for a longer period than other venous access
devices, especially when the reason for their use is
intotal parenteral nutritionlongstanding (such as
s,a chronically ill person). For such indication
mayCath-a-Port, or aPICC line, aHickman linea
be considered because of their smaller infection
risk. Sterile technique is highly important here, as
a line may serve as an entry point for pathogenic
organisms. Additionally, the line itself may become
Staphylococcusinfected with bacteria such as
[3]
negative Staphylococci.-and coagulaseaureus
]editComplications[
Central line insertion may cause several
complications. The benefit expected from their use
should outweigh the risk of those complications.
Pneumothorax
(for central lines placed in thePneumothorax
chest); the incidence is thought to be higher with
subclavian vein catheterization. In catheterization
of the internal jugular vein, the risk of
pneumothorax is minimized by the use
guidance. For experienced clinicians,ultrasoundof
3.1%.-of pneumothorax is about 1.5incidencethe
6. National Institute for Health and ClinicalThe
(UK) and other medical organizationsExcellence
recommend the routine use of ultrasonography to
[4]
minimize complications.
Bloodstream infections
All catheters can introduce bacteria into the
bloodstream, but CVCs are known for occasionally
StaphylococcusandStaphylococcus aureuscausing
-. The problem of central linesepsisepidermidis
associated bloodstream infections (CLABSI) has
They[5]
gained increasing attention in recent years.
(harm) and deaths,morbidityat deal ofcause a gre
and increase health care costs. Historically, a few
CVC infections were considered an acceptable risk
of placing central lines. However, the
groundbreaking work by Dr. Peter Pronovost at
Johns Hopkins Hospital turned that perspective on
Agency forits head. From 2003 to 2006, the
providedHealthcare Research and Quality
$300,000 a year to fund the Comprehensive Unit-
Based Safety Program (CUSP) that helped
participating hospitals in Michigan lower CLABSIs.
By 2012, the project had become a $20 million
Additionally, the Institute[6]
tiative.nationwide ini
7. for Healthcare Improvement (IHI) has done a
tremendous amount of work in improving
hospitals' focus on central line-associated
bloodstream infections (CLABSI), and is working to
decrease the incidence of this particular
complication among US hospitals. The IHI and
CLABSI has identified proper hand washing by the
performing provider, sterile draping over the
person, thorough cleaning of the insertion site,
and daily review for ongoing CVC need as key ways
to decrease infection rate.
The National Patient Safety Goals require
documentation of a checklist for CVC insertion and
Disinfection of intravenous (IV) access ports before
use (scrub the hub). Some literature has suggested
the use of a safer vascular access route,
vascular access, when centralintraosseous (IO)like
lines are not necessary (for example, when central
lines are being placed only for vascular access).
Infection risks were initially thought to be less in
jugular lines, but the decreased rate of infection is
[7]
people.obeseonly seen in
If a central line infection is suspected in a
are taken from both theblood culturesperson,
catheter and a vein elsewhere in the body. If the
8. culture from the central line grows bacteria much
earlier (>2 hours) than the other vein site, the line
is likely infected. Quantitative blood culture is
curate, but this method is not widelyeven more ac
[8]
available.
ed, and occasionallyare usantibioticsGenerally,
the catheter will have to be removed. Infections
Staphylococcusfrombacteremiaresulting in
require removal of the catheter andaureus
antibiotics. If the catheter is removed without
giving antibiotics, 38% of people may still
[9]
.endocarditisdevelop
the,clinical practice guidelineIn a
Centers for Disease Control andAmerican
recommends against routine culturingPrevention
The[10]
on their removal.of central venous lines up
guideline makes several other recommendations
[10]
.line infectionsto prevent
To prevent infection, stringent cleaning of the
-Povidoneite is advised.catheter insertion s
solution is often used for such cleaning,iodine
appears to be twice as effectivechlorhexidinebut
Routine replacement of lines makes[11]
as iodine.
[12]
no difference in preventing infection.
CVCs are a risk factor
9. Thrombosis
CVCs are a risk factoR
)venous thrombosisfor forming blood clots (
deep veinincluding upper extremity
It is thought this risk stems from[14][13]
.thrombosis
activation of clotting substances in the blood by
The risk of[15]
trauma to the vein during placement.
blood clots is higher in a person with cancer, as
cancer is also a risk factor for blood clots. Anti-
clotting drugs such
have been shown tofondaparinuxandheparinas
decrease the incidence of blood clots,
, in a person withdeep vein thrombosisspecifically
Additionally, studies[16]
cancer with central lines.
suggest that short term use of CVCs in the
subclavian vein is less likely to be associated with
blood clots than CVCs placed in the femoral vein in
[17]
cancer patients.-non
MisplacemenT
CVC misplacement is more common when the
anatomy of the person is different or difficult due
[15]
to injury or past surgery.
10. CVCs can be mistakenly placed in an artery during
carotidinsertion (for example, the
when placed in the neckvertebral arteryorartery
when placed in thecommon femoral arteryor
groin). This error can be quickly identified by
special tubing that can show the pressure of the
have a higher pressurearteriescatheter (
). In addition, sending blood samples forveinsthan
,pHacidity, oxygen, and carbon dioxide content (
pO2, pCO2 respectively) can show the
(higher pH/pO2, lowerarterycharacteristics of an
[1]
O2, higher pCO2).(lower pH/pveinpCO2) or
During subclavian vein central line placement, the
catheter can be accidentally pushed into the
internal jugular vein on the same side instead of
the superior vena cava. A chest x-ray is performed
The tip[18]
after insertion to rule out this possibility.
of the catheter can also be misdirected into the
contralateral (opposite side) subclavian vein in the
.superior vena cavaneck, rather than into the
Other complications
Rarely, small amounts of air are sucked into the
thoracic-Intravein as a result of the negative
and insertion technique. Valved insertionpressure
11. airAn]citation needed[
an reduce this risk.devices c
ubbles obstructingis the result of air bembolism
. Air embolisms are a very infrequentblood vessela
complication related to central venous catheter
removal. The threat of air embolism is minimized
VC removalby proper C
[19]
positioning.Trendelenburgwith
(profuse bleeding) and formation ofHemorrhage
(bruise) is slightly more common inhematomaa
[7]
han in others.jugular venous lines t
Uncommonly, the vein can fuse with the artery
after being damaged by insertion of the catheter.
Ultrasound use is efficient at preventing this
[1]
complication.
Insertion
Video of an ultrasound-assisted central line
insertion through the internal jugular vein
12. Before insertion, the patient is first assessed by
reviewing relevant labs and indication for CVC
placement, in order to minimize risks and
complications of the procedure. Next, the area of
skin over the planned insertion site is cleaned.
is applied if necessary. Thelocal anestheticA
location of the vein is identified by landmarks or
. A hollowsound devicesmall ultrawith the use of a
needle is advanced through the skin until blood is
aspirated. The color of the blood and the rate of its
bloodarterialflow help distinguish it from
(suggesting that an artery has been accidentally
punctured). Within North American and Europe,
ultrasound use now represents the gold standard
for central venous access and skills, with
diminishing use of landmark
Recent evidence shows that[21][20]
techniques.
ultrasound-guidance for subclavian vein
eduction in adversecatheterization leads to a r
[22]
events.
SeldingerThe line is then inserted using the
: a blunt guidewire is passed through thechniquete
needle, then the needle is removed. A dilating
device may be passed over the guidewire to
expand the tract. Finally, the central line itself is
then passed over the guidewire, which is then
13. removed. All the lumens of the line are aspirated
(to ensure that they are all positioned inside the
vein) and flushed with
may beray-chest XA[1]
.heparinorsalineeither
performed afterwards to confirm that the line is
andsuperior vena cavapositioned inside the
inadvertently. Onwas causedpneumothoraxno
anteroposterior X-rays, a catheter tip between 55
iscarinamm below the level of theand 29
regarded as acceptable
Electromagnetic tracking can be[23]
placement.
used to verify tip placement and provide guidance
during insertion, obviating the need for the X-ray
afterwards.
A central venous catheter secured to the skin with
suture]]
Chest x-ray with catheter in the right subclavian
vein]]
14.
The outline of superior vena cava on a chest X-ray
is labeled at left.
]editTypes[
There are several types of central venous
[24]
catheters:
Non-tunneled vs. tunneled catheters
Non-tunneled catheters are fixed in place at the
site of insertion, with the catheter and
attachments protruding directly. Commonly used
.ersQuinton cathettunneled catheters include-non
Tunneled catheters are passed under the skin from
the insertion site to a separate exit site. The
catheter and its attachments emerge from
underneath the skin. The exit site is typically
located in the chest, making the access ports less
visible than catheters that protrude directly from
the neck. Passing the catheter under the skin helps
to prevent infection and provides stability.
Commonly used tunneled catheters
15. GroshongandHickman cathetersinclude
.catheters
Implanted port
Port (medical)Main article:
Illustration of a venous access port.
Implanted port
is similar to a tunneled catheter but is leftportA
entirely under the skin. Medicines are injected
through the skin into the catheter. Some
implanted ports contain a small reservoir that can
16. be refilled in the same way. After being filled, the
reservoir slowly releases the medicine into the
bloodstream. An implanted port is less obvious
than a tunneled catheter and requires little daily
care. It has less impact on a person's activities than
a PICC line or a tunneled catheter. Surgically
implanted infusion ports are placed below the
clavicle (infraclavicular fossa), with the catheter
) through aright atriumhreaded into the heart (t
large vein. Once implanted, the port is accessed
via noncoring "Huber" needles inserted through
the skin. The health care provider may need to use
topical anesthetic before accessing the port. Ports
can be used for medications, chemotherapy, and
blood. As ports are located completely under the
skin, they are easier to maintain and have a lower
[1]
theters.risk of infection than CVC or PICC ca
Ports are typically used on patients requiring only
occasional venous access over a long duration
course of therapy. Since the port must be accessed
using a needle, if venous access is required on a
frequent basis a catheter having external access is
[1]
more commonly used.
17. PICC line
PICCcentral catheter, orA peripherally inserted
(pronounced "pick"), is a central venousline
catheter inserted into a vein in the arm (via
veins) rather than a vein incephalicorbasilicthe
the neck or chest. The tip is positioned in the
[1]
superior vena cava.
Technical description
Triluminal catheter
Depending on use, catheters may have a
) or(a "monoluminal catheter"lumensingle
multiple lumens. A catheter with two lumens is
"biluminal", three "triluminal". Up to 4 or 5 lumens
may be used, allowing multiple drug infusions to
be delivered and monitored simultaneously.
The catheter is held in place by an adhesive
dressing, suture, or staple which is covered by an
18. occlusive dressing. Regular flushing with saline or
containing solution keeps the line open-heparina
. There is no evidence thatblood clotsand prevents
heparin is better than saline at preventing blood
Certain lines are impregnated with5][2
clots.
containing substances-antibiotics, silver
)silver sulfadiazine(specifically
[26]
to reduce infection risk.chlorhexidineand/or
term central lines are-Specific types of long
, which require clamps toHickman cathetersthe
make sure that the valve is closed, and Groshong
catheters, which have a valve that opens as fluid is
withdrawn or infused and remains closed when
not in use. Hickman lines also have a "cuff" under
citation[
the skin, to prevent bacterial migration.
The cuff also causes tissue ingrowth into the]needed
device for long term securement.
![central venoussaturation"), and measure
[2][1]
.pressure
]editMedical uses[
Central line equipment, in order of typical usage:
1.local anestheticSyringe with
2.is neededvenous cutdownScalpel in case
3.guidanceultrasoundSterile gel for
4.) on syringeGaIntroducer needle (here 18
to detect backflow of blood uponsalinewith
vein penetration
5.Guide wire
6.Tissue dilator
7.)Gadwelling catheter (here 16In
8.Additional fasteners, and corresponding
surgical thread
9.Dressing](data:image/gif;base64,R0lGODlhAQABAIAAAAAAAP///yH5BAEAAAAALAAAAAABAAEAAAIBRAA7)