Downloaded 21 times

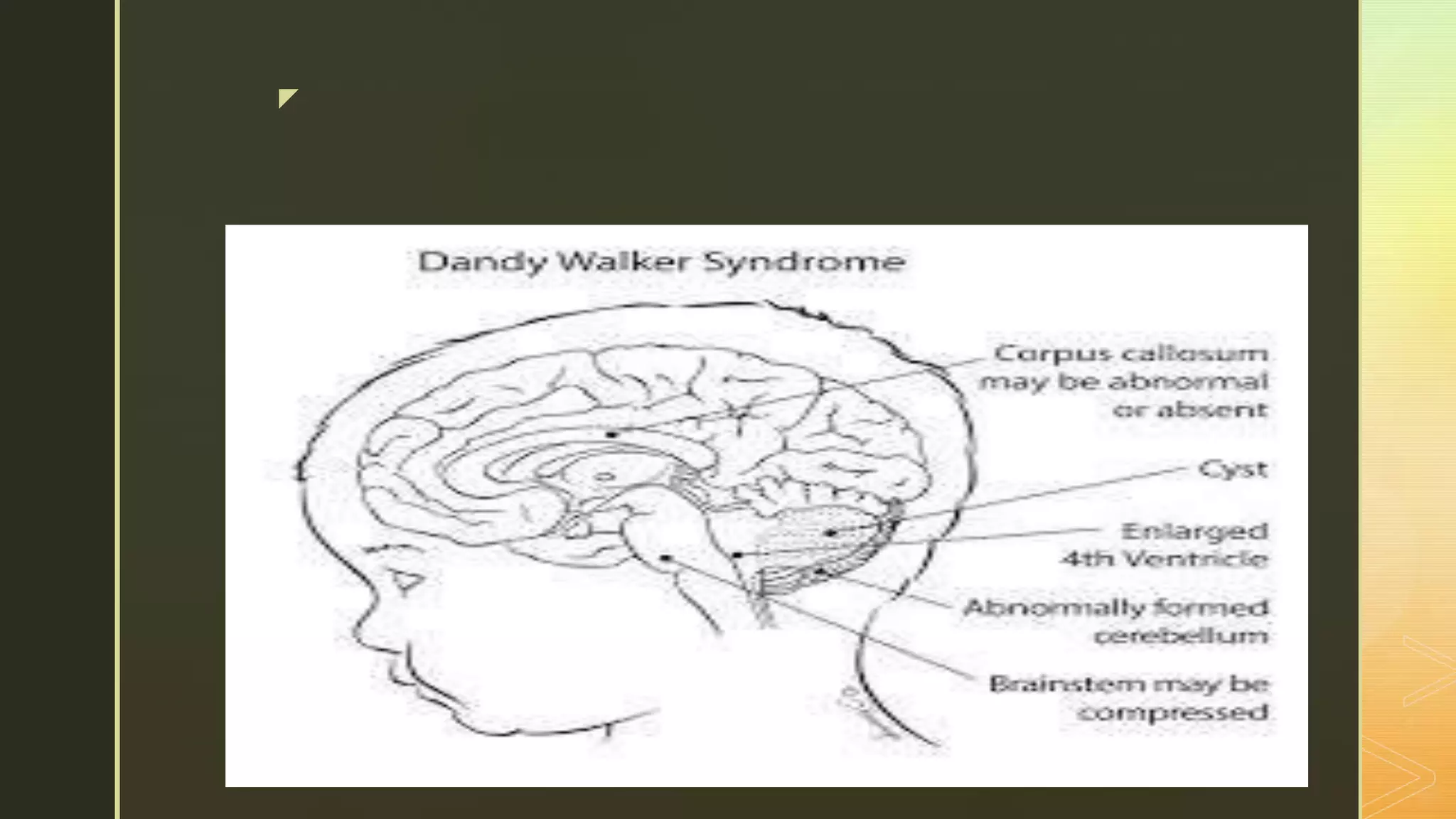

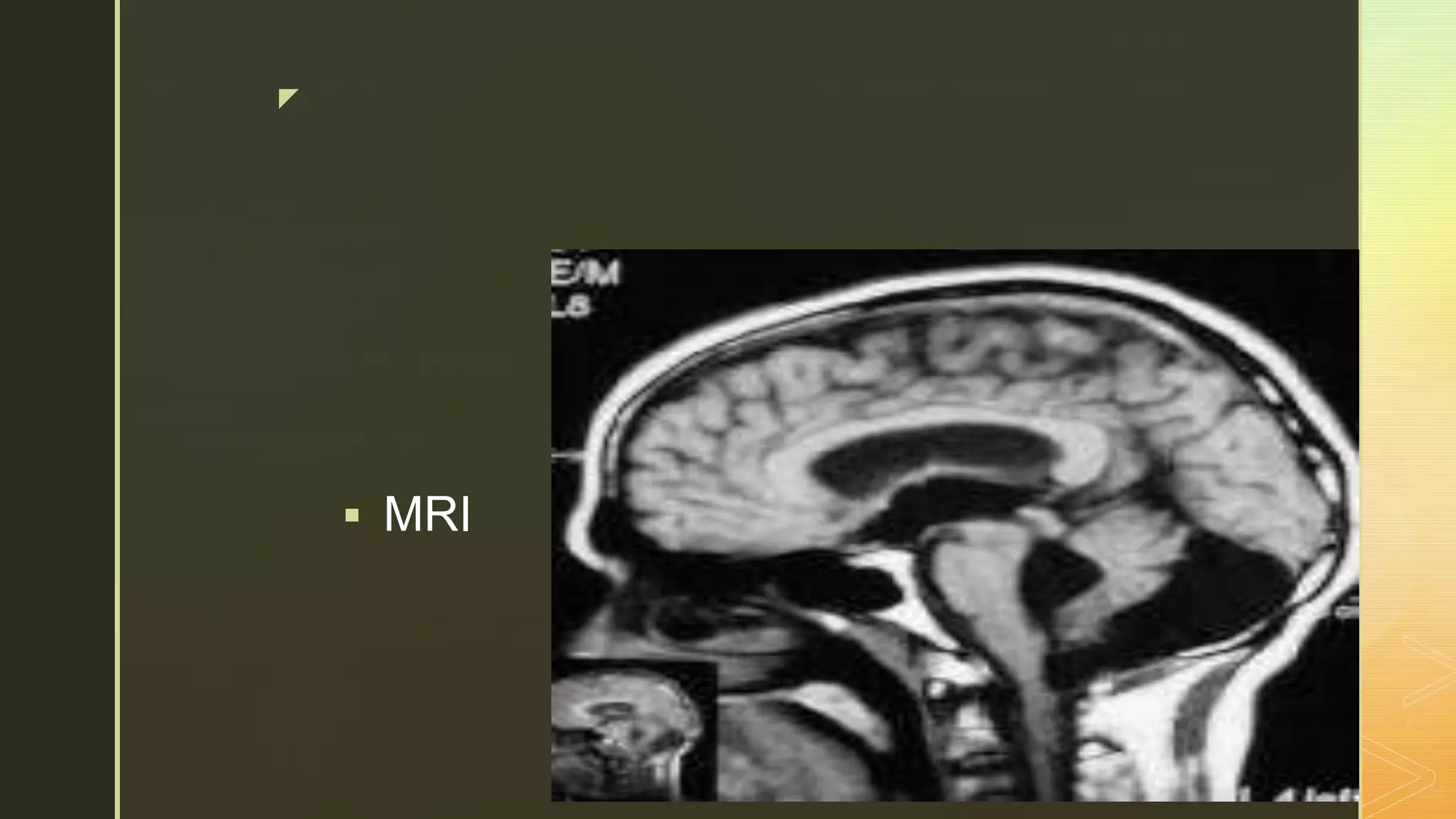
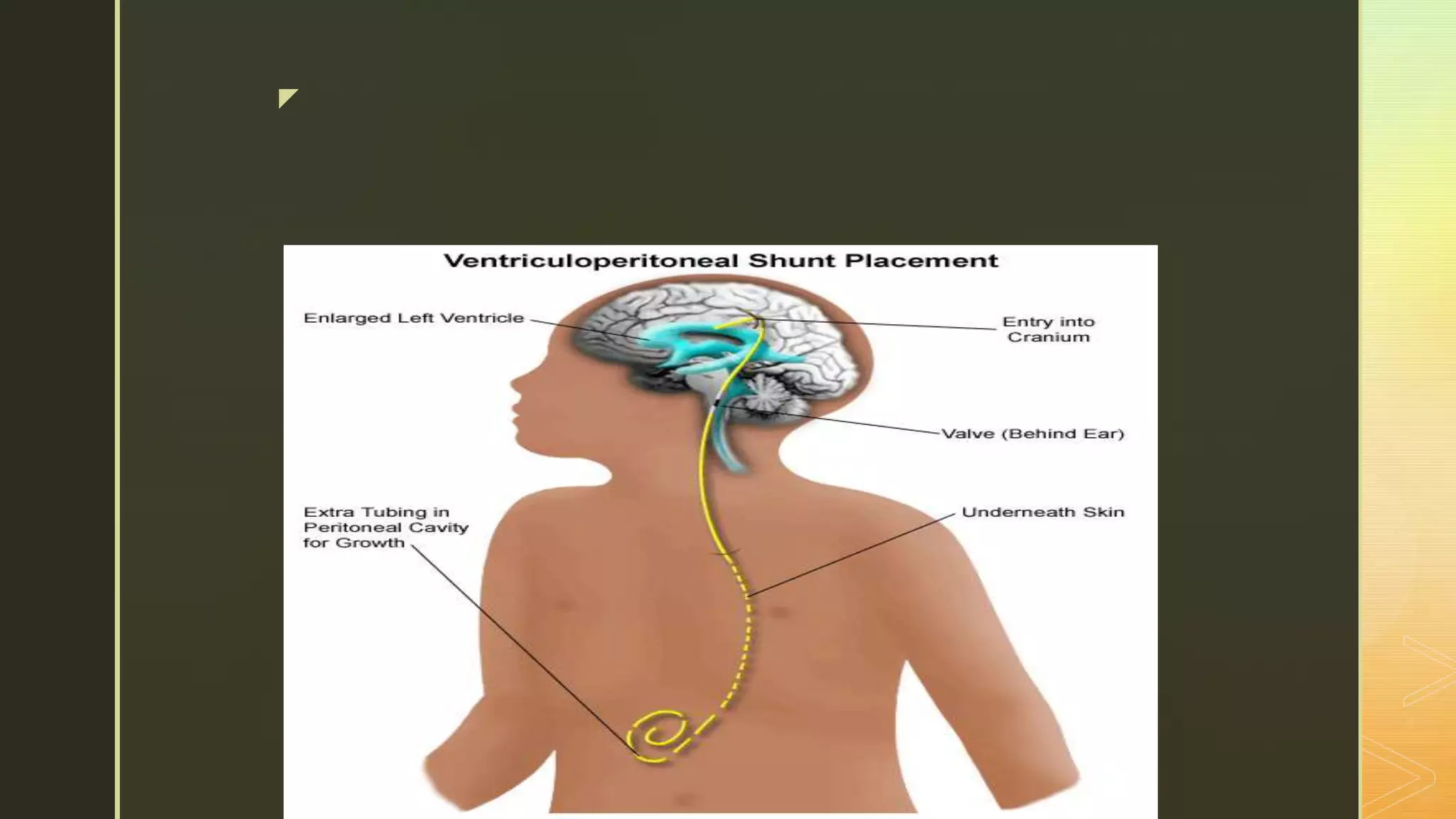


Dandy Walker Malformation is a congenital brain malformation characterized by 3 key features: an enlarged posterior fossa, an abnormal or absent cerebellar vermis, and a cyst in the fourth ventricle. It occurs due to genetic and environmental factors affecting fetal brain development. Patients experience developmental delays, motor problems, seizures, and other issues depending on severity. Diagnosis is via ultrasound, MRI or CT scan. Treatment involves surgery to address hydrocephalus and medications to control seizures. Prognosis depends on defect severity but early treatment can improve outcomes.










































































