Download as PDF, PPTX











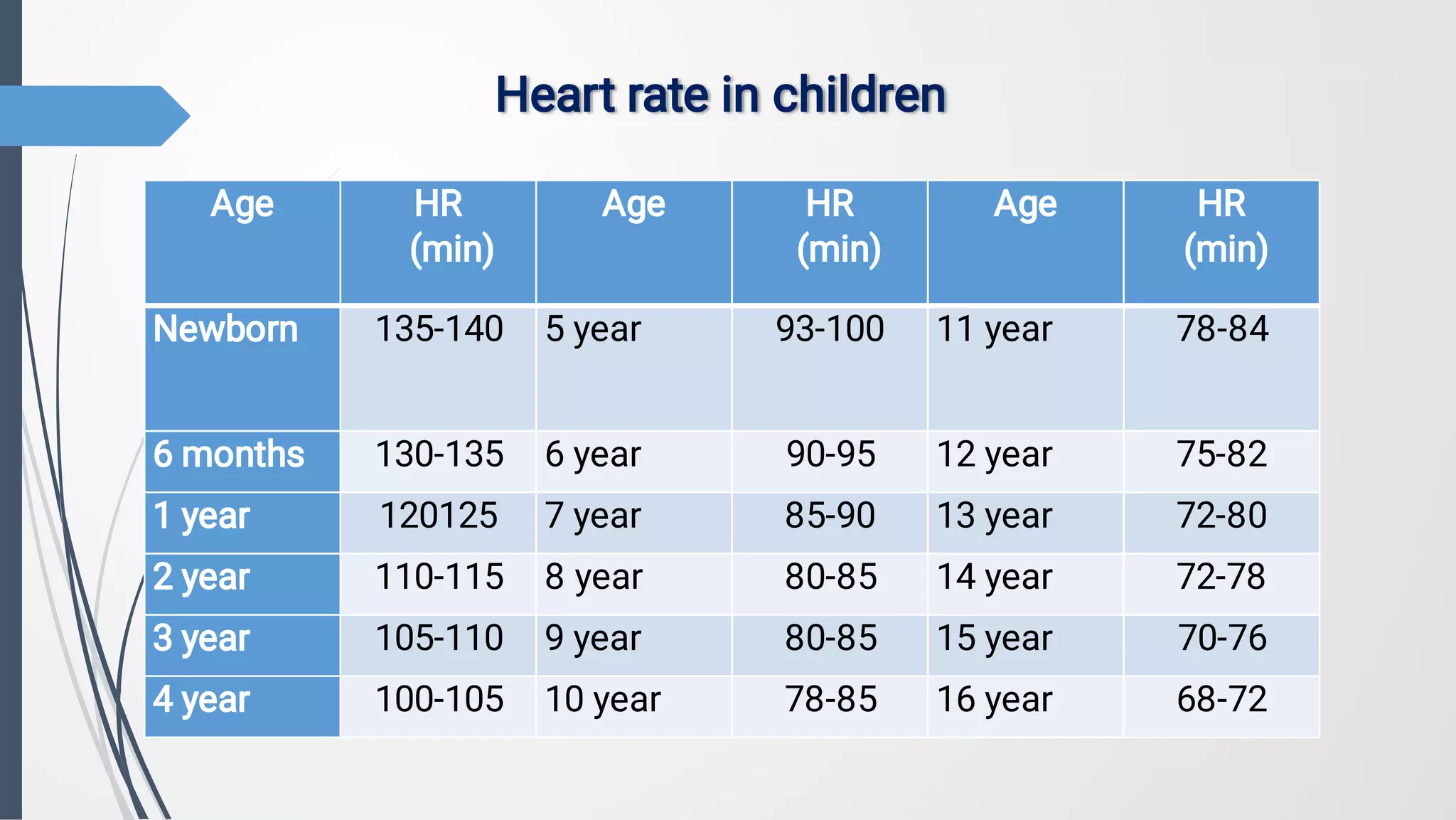
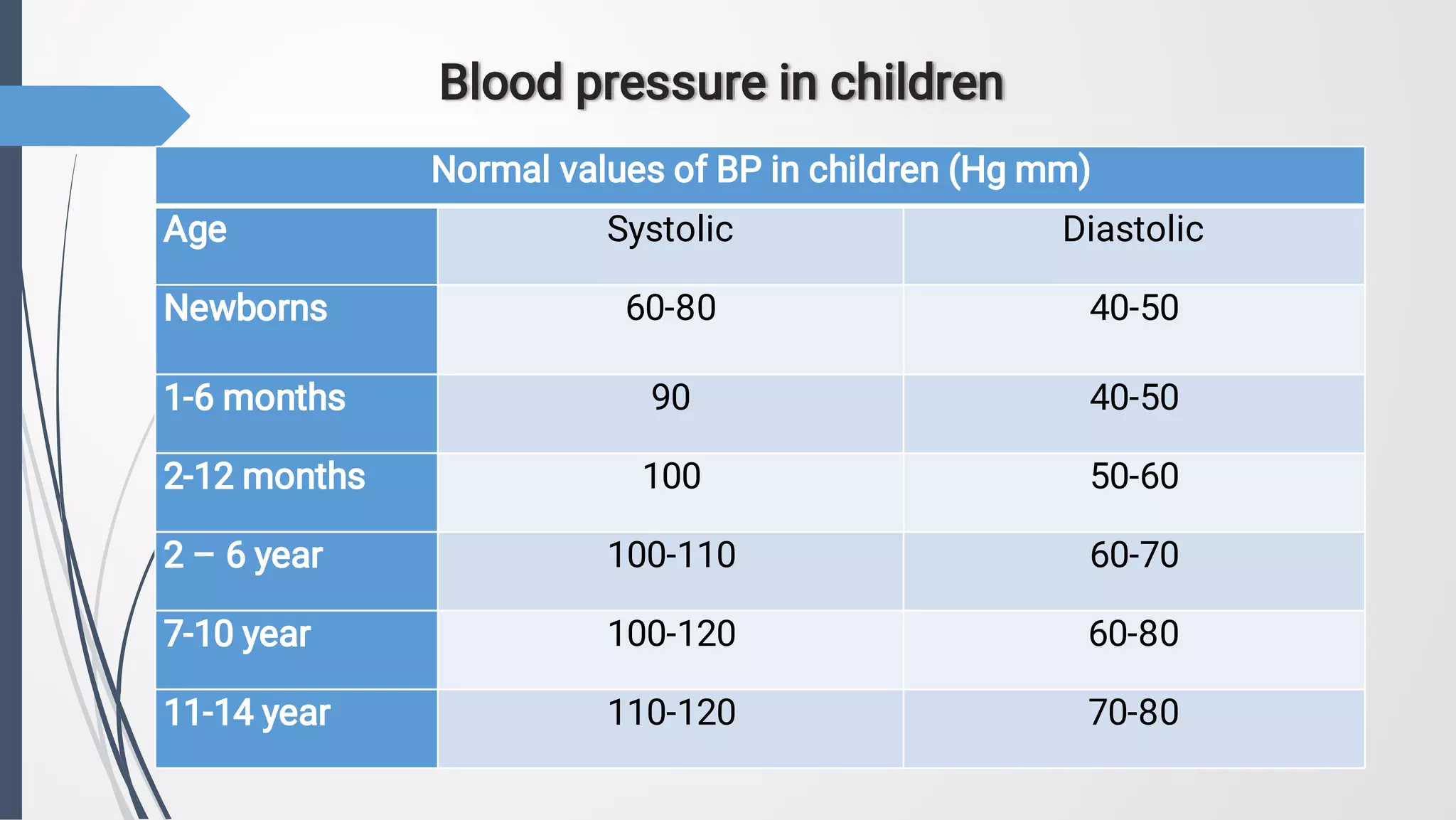
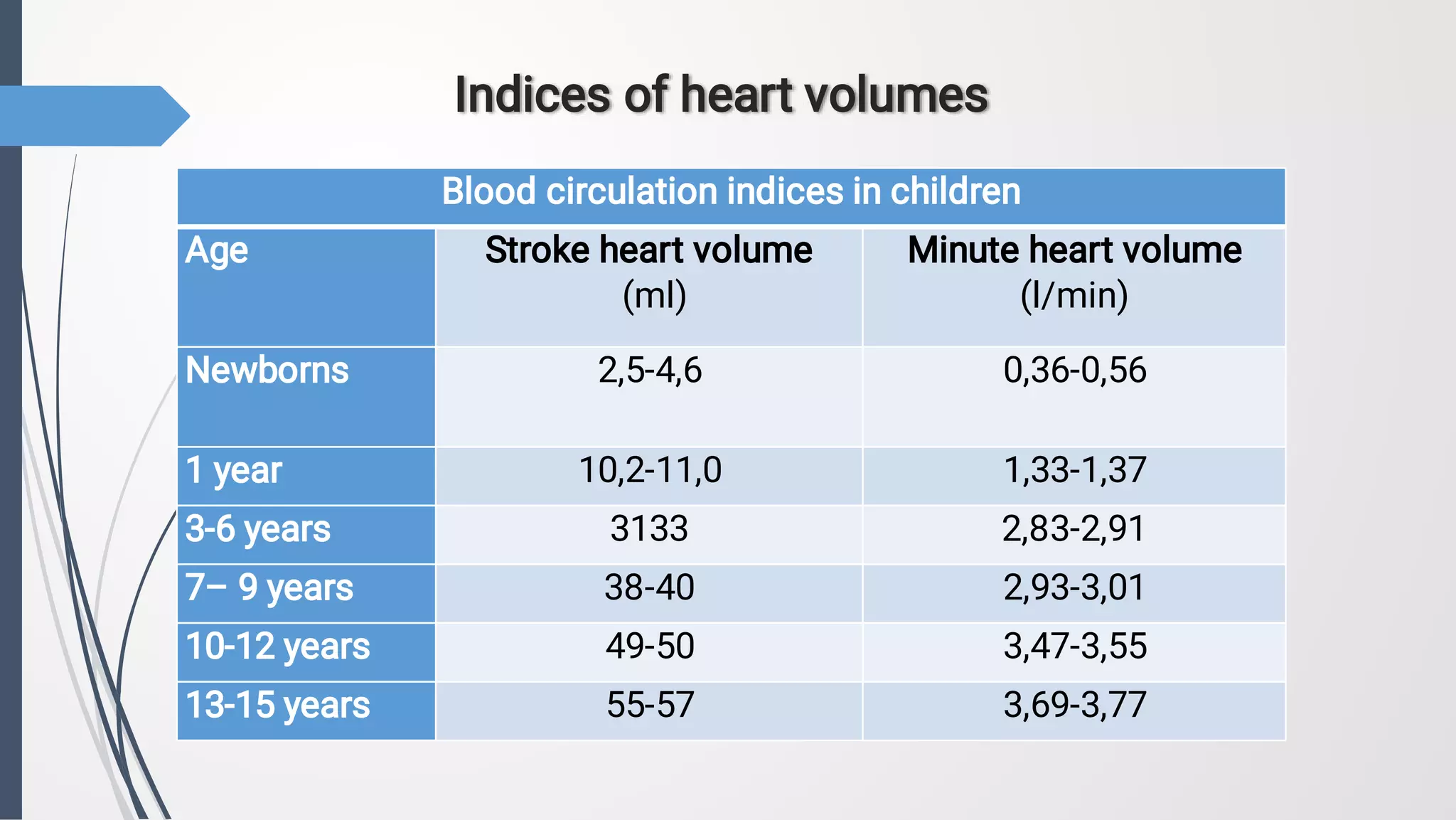













































































1. The document discusses anatomical and physiological features of the cardiovascular system in children. It covers stages of heart and blood vessel formation prenatally, closure of the fetal circulatory system after birth, and features of the heart and circulation at different ages. 2. The document also discusses methods for objectively investigating the cardiovascular system in children, including inspection, palpation, percussion, auscultation, electrocardiography, chest x-ray, echocardiography, and functional tests. Normal ranges are provided for several cardiovascular parameters at different pediatric ages. 3. The document classifies congenital heart diseases and discusses hemodynamic changes and clinical presentations of some common defects, including those with increased or decreased























































































