Downloaded 99 times

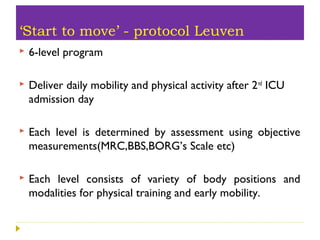
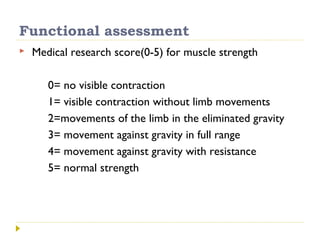

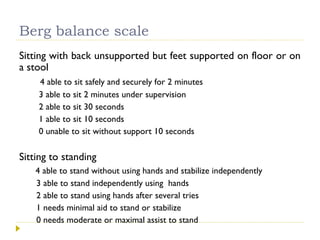
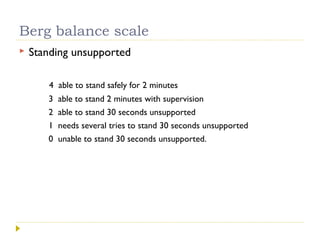
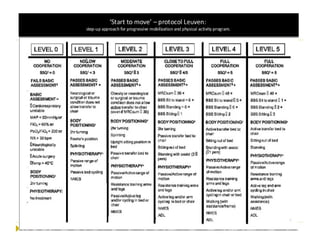

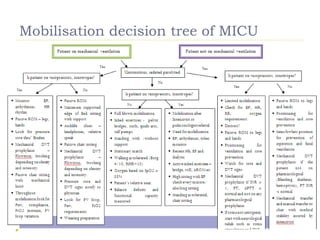
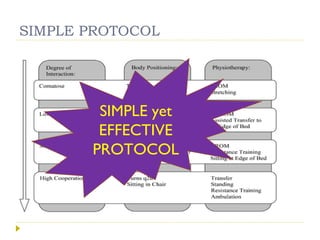




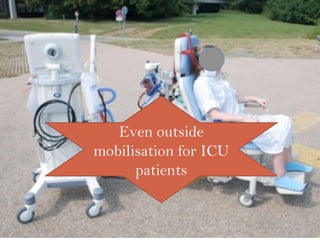



This document discusses mobilization for patients in the intensive care unit (ICU). It defines mobilization as any activity done regularly in the ICU, either passively or actively, to improve hemodynamics, reverse effects of bed rest, and more. Common mobilization forms mentioned are active, passive, manual, and mechanical exercises. The goals of mobilization are to reduce complications from critical illness and bed rest, improve outcomes, and aid recovery. Factors to consider for safe and effective mobilization are the patient's medical stability and functional ability based on assessments. Mobilization should be a team effort and follow a stepwise protocol tailored to the individual patient.
















































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)


















