Downloaded 133 times
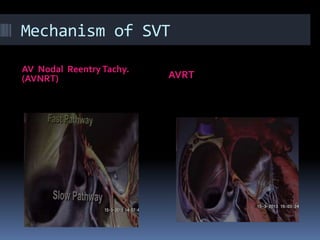
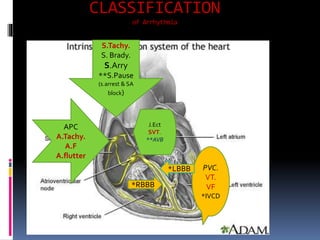
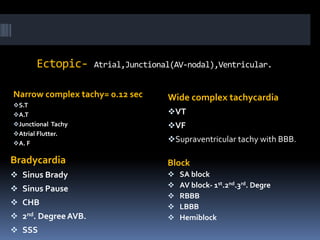
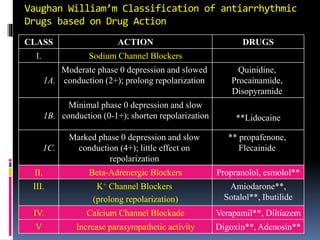
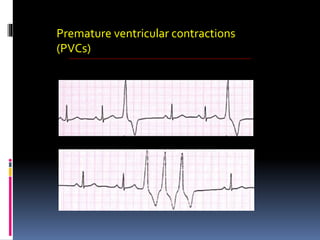
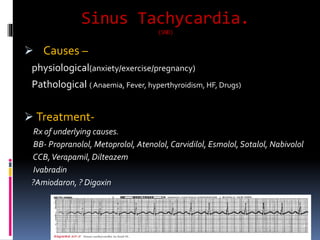
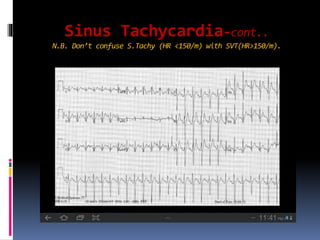
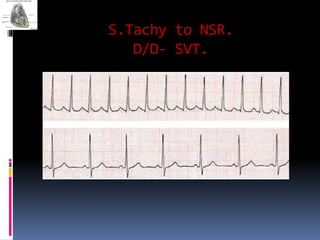
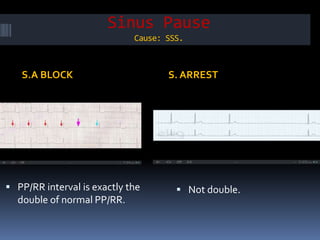
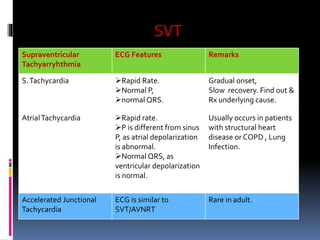
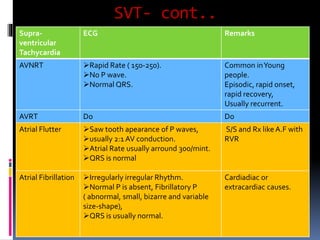
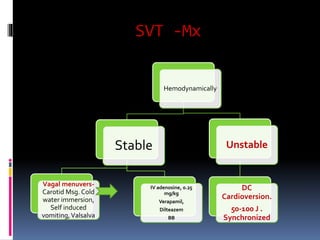
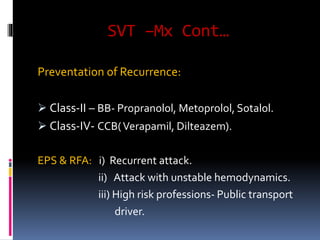
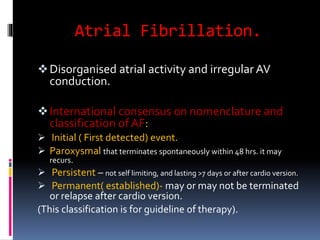
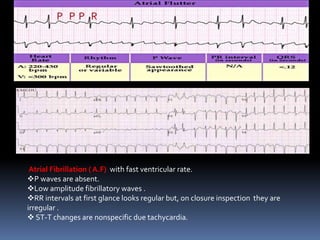




This document provides an overview of cardiac arrhythmias including definitions, mechanisms, classifications, and ECG patterns. It discusses abnormal heart rhythms in terms of rate, rhythm, and conduction abnormalities. Common arrhythmias like sinus tachycardia, atrial fibrillation, ventricular tachycardia, and heart blocks are described. Treatment options for arrhythmias include medications, cardioversion, ablation, and pacemakers. Antiarrhythmic drug classifications and their mechanisms of action are also reviewed.












































































