Downloaded 52 times
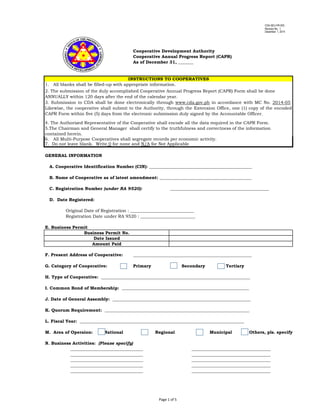





The document outlines the Cooperative Annual Progress Report (CAPR) requirements and includes various sections for cooperatives to provide essential information such as identification numbers, registration details, business activities, and membership details. It specifies the procedure for submitting the CAPR electronically to the Cooperative Development Authority (CDA) along with additional documentation, emphasizing the importance of accuracy and completeness. The report encompasses critical financial and operational data, including capitalization and tax information, aimed at ensuring compliance with regulatory standards.