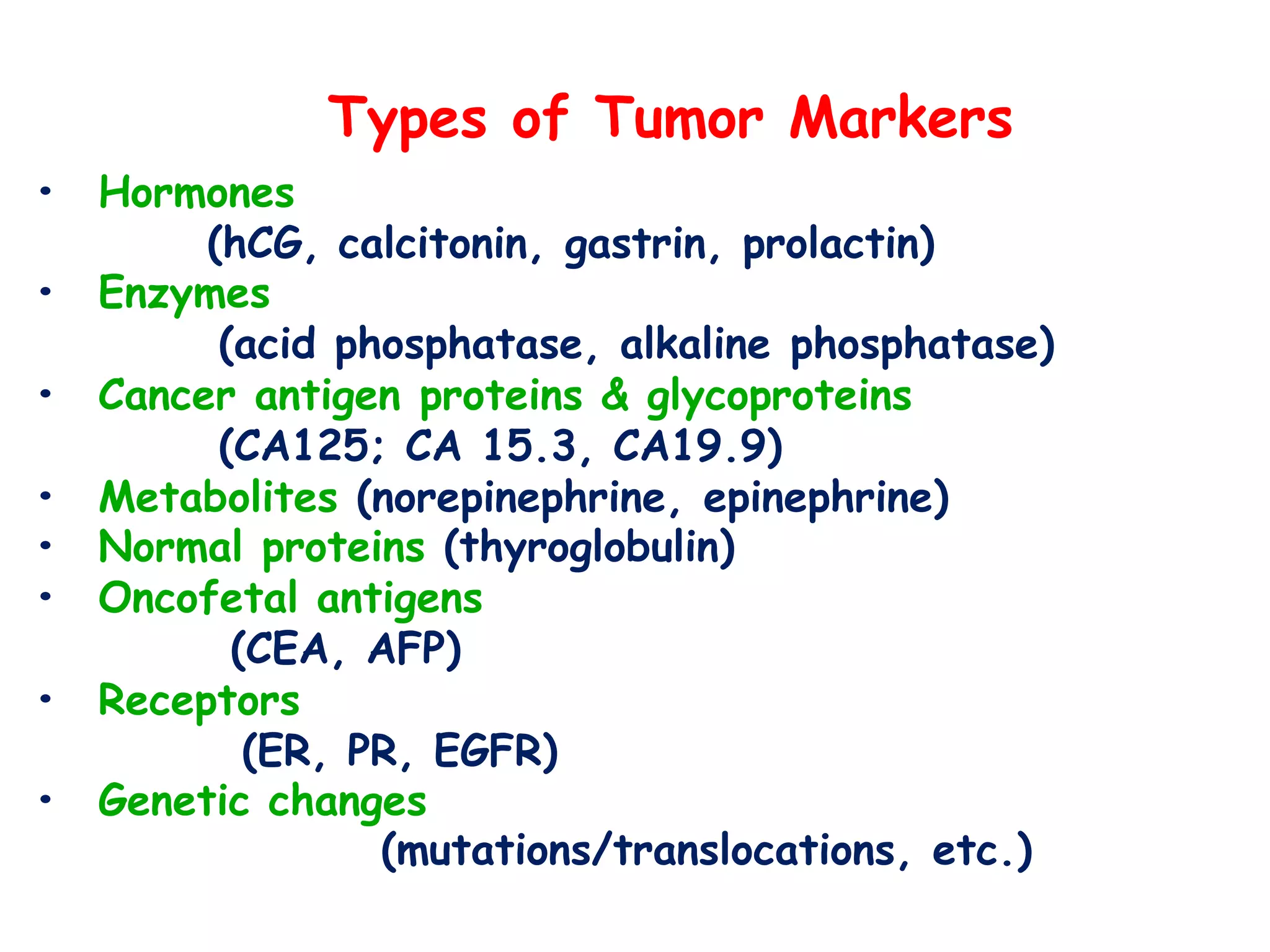
Cancer is the second leading cause of death worldwide after cardiovascular disease. In India, an estimated 2.25 million people are living with cancer, with over 11 lakh new cases registered annually. Some key statistics for India include one woman dying of cervical cancer every 8 minutes and two women dying of breast cancer for every one diagnosed. Tumor markers are substances produced by cancerous tissues or the body in response to cancer that can help detect or monitor cancer. Some common tumor markers are CEA, AFP, CA125, and PSA. Tumor markers can be used for screening, diagnosis, staging, prognosis, and monitoring treatment effectiveness and recurrence. Characteristics of ideal tumor markers include cancer specificity, high sensitivity and specificity for detection