Downloaded 41 times
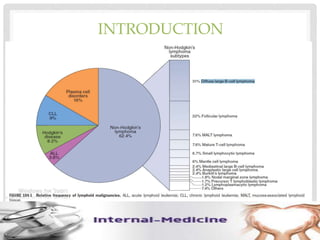
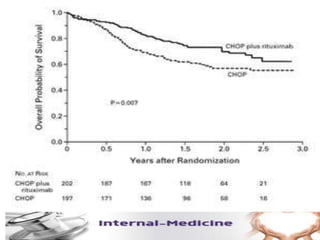
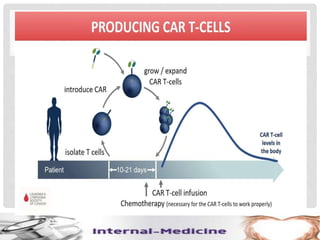
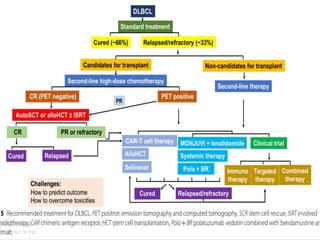

This document provides an overview of diffuse large B-cell lymphoma (DLBCL), including epidemiology, risk factors, presentation, histology, genetics, therapy, and treatment options. DLBCL is the most common subtype of non-Hodgkin lymphoma. The standard first-line treatment is rituximab combined with cyclophosphamide, doxorubicin, vincristine, and prednisone (R-CHOP). For early stage disease, options include full chemotherapy or abbreviated chemotherapy with radiation. Advanced disease is treated with full chemotherapy. Refractory cases may be treated with newer agents or CAR T-cell therapy.








































































![Cells and Organs of immune system [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/cellsandorgansofimmunesystemautosaved-260123152717-ea0cb261-thumbnail.jpg?width=640&height=640&fit=bounds)









