This document discusses endometrial carcinoma (cancer of the uterus). It covers the epidemiology, risk factors, types/classification, diagnosis, staging, treatment and prognosis. Some key points:
- It is the 3rd most common female cancer in India, occurring most often in post-menopausal women aged 60-70. The 5-year survival rate is approximately 75%.
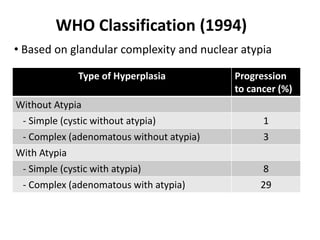
- There are two main types - Type 1 is associated with estrogen exposure, is lower grade, and has a better prognosis. Type 2 occurs without estrogen stimulation, is higher grade and has a poorer prognosis.
- Risk factors include family history, nulliparity, early menarche/late menopause, obesity,













































![APPROACH TO FEVER IN PEDIATRICS[1].pptTT](https://cdn.slidesharecdn.com/ss_thumbnails/approachtofeverinpediatrics1-260125081456-d559e079-thumbnail.jpg?width=640&height=640&fit=bounds)
