Download to read offline




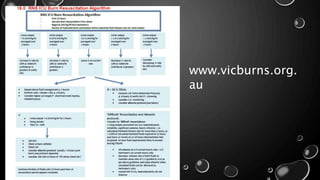



The document discusses crucial considerations in managing burn shock, emphasizing the need for accurate assessment and tissue perfusion preservation while avoiding over-resuscitation. It highlights the complexities associated with patients of extreme ages, those with significant inhalation injuries, and extensive burns, along with comorbidities. Early referral and multi-faceted care approaches are advised to improve outcomes and manage complications effectively.



































































