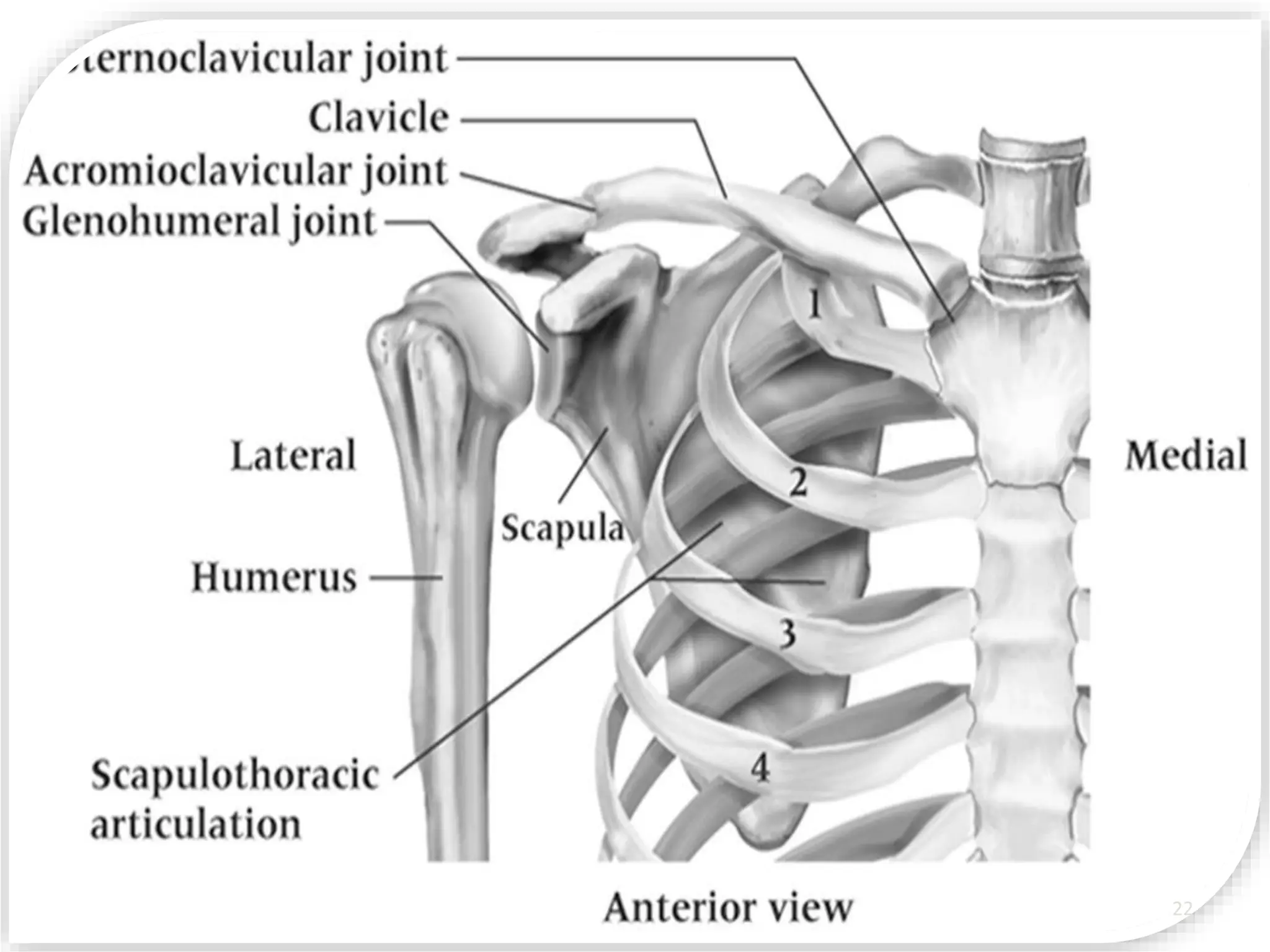
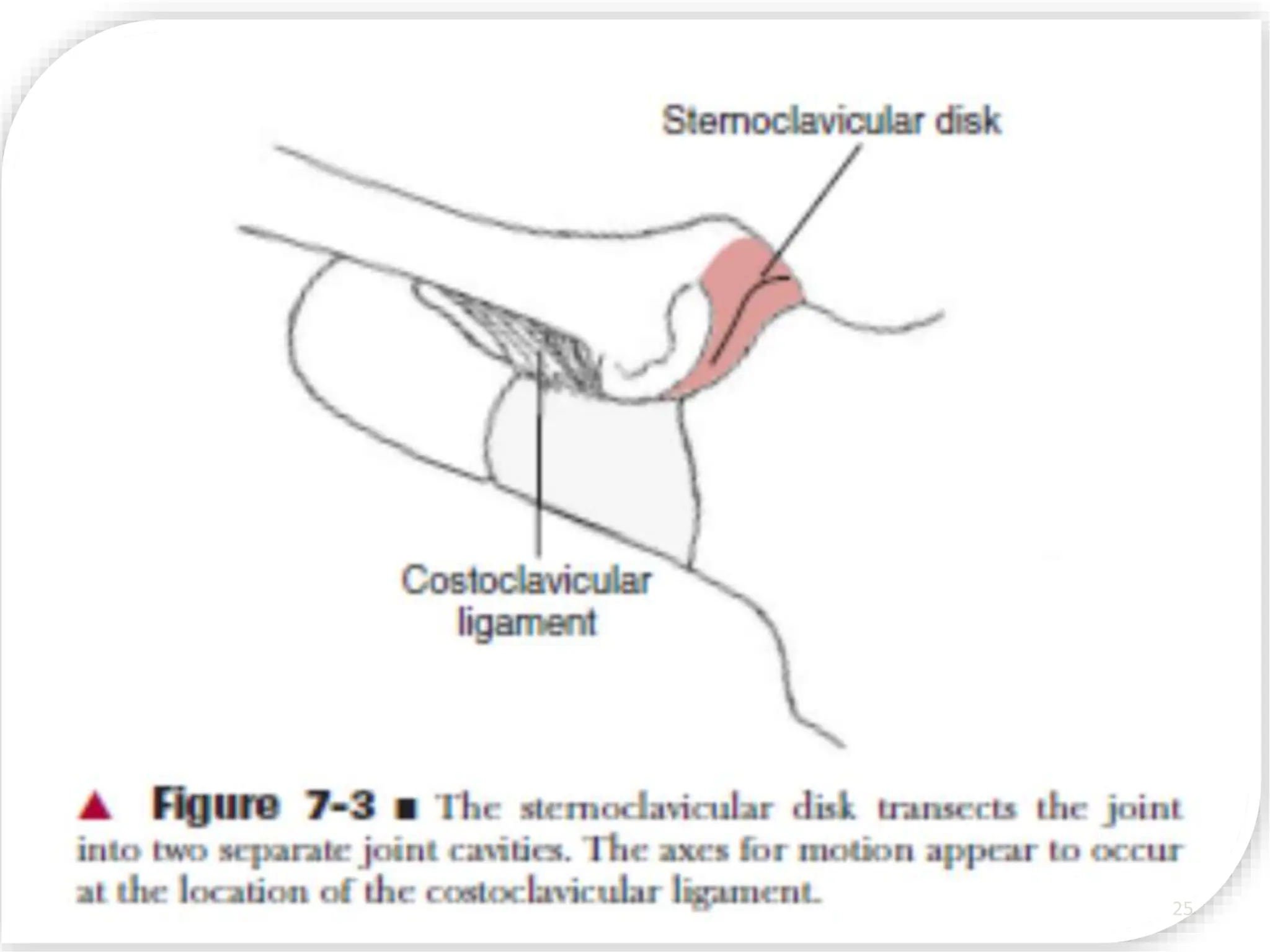
This document provides an overview of the biomechanics of the shoulder complex. It defines key terms in biomechanics and describes the structures that make up the shoulder complex, including the bones (osteology), joints, ligaments, and muscles. It explains the kinetics and kinematics of the glenohumeral joint and surrounding structures, describing their motions and biomechanical functions including providing stability to the shoulder. Pathologies that can affect the shoulder complex are also briefly mentioned.