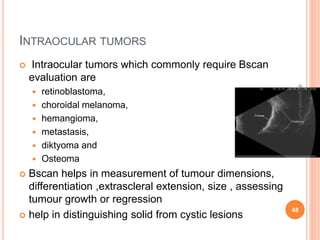
B-scan ultrasonography provides two-dimensional images of ocular structures through the use of high frequency sound waves. It can be used to evaluate a variety of conditions, including retinal detachment, vitreous hemorrhage, intraocular tumors, and trauma. Retinal detachment appears on B-scan as an echogenic membrane attached to the optic nerve head, while vitreous hemorrhage shows as fine echo opacities within the vitreous cavity. B-scan is useful for assessing patients with dense cataracts or other opaque media by allowing visualization of the posterior segment.