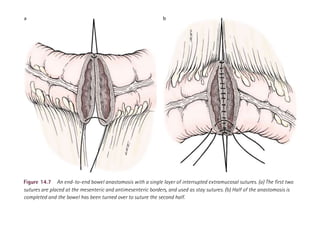
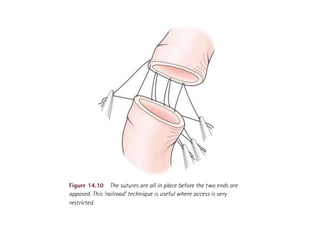
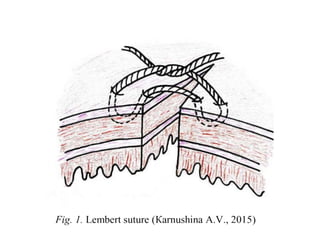
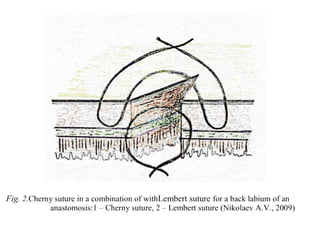
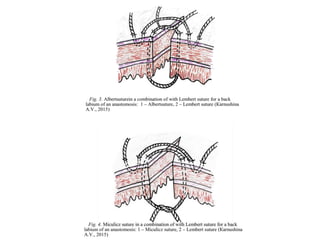
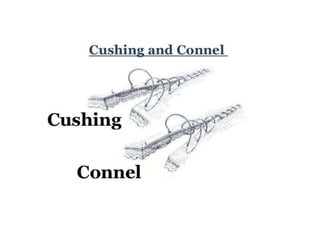
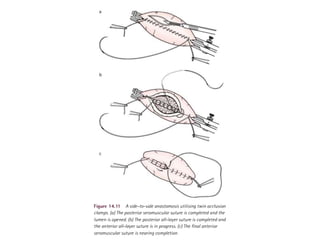
This document discusses various techniques for performing anastomoses during gastrointestinal surgery. It notes important factors to consider like blood supply, tension, and diameter. For colorectal and small bowel anastomoses, it recommends using slowly absorbable monofilament sutures with a 5mm bite from the margin. A single-layer inverting anastomosis is preferred for colorectal procedures as it is less time-consuming and reduces inflammation. Advantages of the single-row suture technique include faster performance and less trauma. End-to-end anastomoses should include the muscular mucosa. Side-to-side anastomoses employ a four-layer technique with separate sutures for the posterior