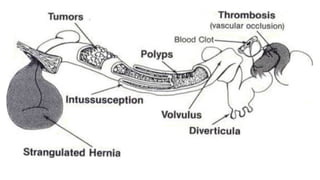
Indication of resection
1)Vascularcompromise leading to bowel gangrene
2)Malignancy
3)Benign conditions like intestinal polyps, intussusception, ca u s in g intestinal obstruction,not responsive to
conservative therapy.
4)Strictures following infections like tuberculosis
5)Perforations at multiple sites of bowel
6)Large perforations which cannot be repaired by primary closure
7)Radiation enteritis complicated with bleeding, stricture, or perforation
8)Inflammatory bowel disease, ulcerative colitis refractory / not responding to medical therapy or with
complication.
9) Hirschsprung disease: Subtotal colectomy may be performed if the disease is refractory to conservative
therapy
5.
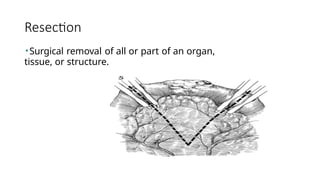
Anastomosis
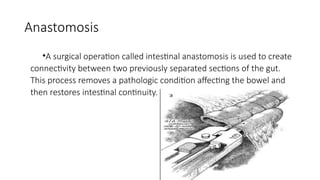
•A surgical operationcalled intestinal anastomosis is used to create
connectivity between two previously separated sections of the gut.
This process removes a pathologic condition affecting the bowel and
then restores intestinal continuity.
6.
Indications for intestinalanastomosis can be broadly divided into three
categories:
1) To restore bowel continuity after resection of diseased bowel .
2)To bypass of unresectable diseased bowel.
3)In Traumatic disruption of bowel continuity.
7.
• Bypass ofunresectable diseased bowel is performed in following
settings:
1)Locally advanced tumor of bowel causing obstruction
2)Metastatic disease producing intestinal obstruction
3) Congenital obstruction of bowel.
4) Poor general condition of the patient.
8.
•Features of anideal anastomosis
1. There is no chance of leakage
2. No damage to the vascular supply
3. Absence of luminal narrowing
4. Early functional achievement
5. Quick recovery and brief hospitalization for patients
9.
Contraindications of Anastomosis
•Contraindications to intestinal anastomosis include conditions in which
there is high risk of anastomotic leak, such as the following:-
1)Patient suffering from Severe sepsis
2)Patient with Poor nutritional status
3)Disseminated malignancy throughout peritoneum
4)Viability of bowel in doubt
5)Faecal contamination or frank peritonitis
6)Unhealthy bowel condition
10.
Healing of ananastomosis
• Occurs in 3 phases
1. Acute inflammatory phase
2. Proliferative phase
3. Remodelling or maturation phase
• Acute inflammatory phase is the early phase of healing of an anastomosis. Occurs within 0-4 days
after the surgery. There is no intrinsic cohesion between the two ends. There is accumulation of
mediators of inflammation at the anastomotic site producing an acute inflammatory response.
• Proliferative phase Occurs 3 to 14 days after the surgery. It is the phase of accumulation and
proliferation of fibroblasts. This leads to collagen formation.
• Maturation phase occurs 10 days after the anastomosis. This phase leads to stability and strength to
the site. Almost 90% of the tensile strength is gained in 6 months
11.
Principles of anastomosis
1.There should be adequate arterial supply and venous drainage
2. Anastomosis should be between two ends free from disease
3. Always distal obstruction should be ruled out before joining the ends
4. Direction of peristaltic waves should be considered
5. There should not be any tension, twisting or excessive constriction while
anastomosing
6. Avoid back pressure and stagnation
12.
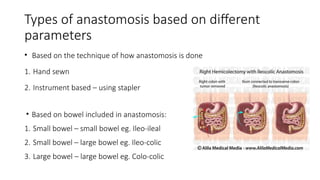
Types of anastomosisbased on different
parameters
• Based on the technique of how anastomosis is done
1. Hand sewn
2. Instrument based – using stapler
• Based on bowel included in anastomosis:
1. Small bowel – small bowel eg. Ileo-ileal
2. Small bowel – large bowel eg. Ileo-colic
3. Large bowel – large bowel eg. Colo-colic
13.
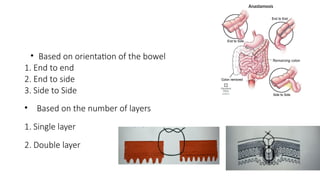
• Based onorientation of the bowel
1. End to end
2. End to side
3. Side to Side
• Based on the number of layers
1. Single layer
2. Double layer
14.
• Sutured anastomosis(hand—sewn technique)commonly used because
of the availability and affordability of suture materials and familiarity
with the procedure.
• Stapling definitely reduces the operative time and facilitated the ease of
doing the procedure, especially in low colorectal anastomosis.
15.
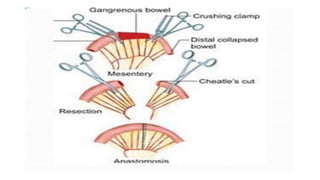
Bowel Resection
• Theportion of bowel to be resected should be adequately mobilized. The bowel should be checked for
any distal obstruction.
• After mobilization of the bowel, the next step is division of the mesentery.
Principles to be followed in division of the mesentery include the following:
• Transillumination to identify mesenteric blood vessels
• Isolation of vessels by dividing surrounding fat
• Division between clamps
• Ligation with suitable sutures to prevent knot slippage
• On-needle transfixation of large vascular pedicles with nonabsorbable sutures is a safer method. Bleeding
or hematoma formation within the leaves of mesentery should be avoided, and preservation of vascular
arcade to the bowel ends should be ensured so as to have satisfactory vascularity of the anastomosed
bowel. As hematoma formation can will disrupt the blood supply to the anastomotic site and cause
mucosal ulceration which leads to distal ischemia. Alternatively, the mesentery can be divided with an
ultrasonic scalpel.
16.
• The nextstep is division of the bowel. This is done by applying a noncrushing clamp on the bowel
end used for anastomosis and applying crushing clamps on the bowel to be resected so that the
intraluminal contents of the resected bowel do not contaminate the peritoneal cavity. Clamps are
applied from the antimesenteric end, and care should be taken to avoid crushing of the
mesentery.
• The bowel is divided with a knife close to the crushing clamp so as to preserve adequate bowel
length distal to a noncrushing clamp for anastomosis. The direction of division is oblique to ensure
an adequate lumen and to maintain a longer length of the mesenteric end as compared with the
antimesenteric end. The specimen is removed with clamps in situ.
• While dividing the bowel , we should divide the bowel well in advance, then wash peritoneal
cavity for minimum 20 minutes then we should go for anastomosis
• Care should be taken to avoid spillage of enteric contents during bowel division. Alternatively,
bowel division can also done with a linear cutting (gastrointestinal anastomosis [GIA]) stapler,
which divides and seals two cut ends simultaneously, thereby preventing fecal contamination as
fecal contamination is a negative factor for intestinal anastomosis
18.
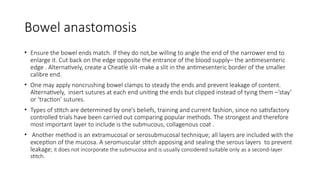
Bowel anastomosis
• Ensurethe bowel ends match. If they do not,be willing to angle the end of the narrower end to
enlarge it. Cut back on the edge opposite the entrance of the blood supply– the antimesenteric
edge . Alternatively, create a Cheatle slit-make a slit in the antimesenteric border of the smaller
calibre end.
• One may apply noncrushing bowel clamps to steady the ends and prevent leakage of content.
Alternatively, insert sutures at each end uniting the ends but clipped instead of tying them –’stay’
or ‘traction’ sutures.
• Types of stitch are determined by one’s beliefs, training and current fashion, since no satisfactory
controlled trials have been carried out comparing popular methods. The strongest and therefore
most important layer to include is the submucous, collagenous coat .
• Another method is an extramucosal or serosubmucosal technique; all layers are included with the
exception of the mucosa. A seromuscular stitch apposing and sealing the serous layers to prevent
leakage; it does not incorporate the submucosa and is usually considered suitable only as a second-layer
stitch.
20.
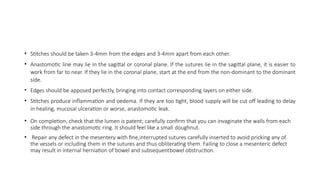
• Stitches shouldbe taken 3-4mm from the edges and 3-4mm apart from each other.
• Anastomotic line may lie in the sagittal or coronal plane. If the sutures lie in the sagittal plane, it is easier to
work from far to near. If they lie in the coronal plane, start at the end from the non-dominant to the dominant
side.
• Edges should be apposed perfectly, bringing into contact corresponding layers on either side.
• Stitches produce inflammation and oedema. If they are too tight, blood supply will be cut off leading to delay
in healing, mucosal ulceration or worse, anastomotic leak.
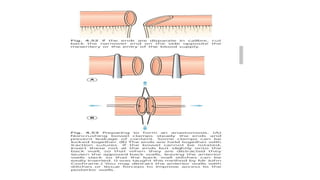
• On completion, check that the lumen is patent; carefully confirm that you can invaginate the walls from each
side through the anastomotic ring. It should feel like a small doughnut.
• Repair any defect in the mesentery with fine,interrupted sutures carefully inserted to avoid pricking any of
the vessels or including them in the sutures and thus obliterating them. Failing to close a mesenteric defect
may result in internal herniation of bowel and subsequentbowel obstruction.
21.
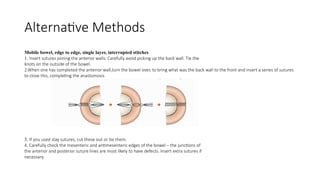
Alternative Methods
Mobile bowel,edge to edge, single layer, interrupted stitches
1. Insert sutures joining the anterior walls. Carefully avoid picking up the back wall. Tie the
knots on the outside of the bowel.
2.When one has completed the anterior wall,turn the bowel over, to bring what was the back wall to the front and insert a series of sutures
to close this, completing the anastomosis
3. If you used stay sutures, cut these out or tie them.
4. Carefully check the mesenteric and antimesenteric edges of the bowel – the junctions of
the anterior and posterior suture lines are most likely to have defects. Insert extra sutures if
necessary.
22.
Edge to edge,single layer, continuous stitches
• Starting on the back wall, insert a stitch at one end from outside in
on one side, inside: out on the other side and tie it. Clip the short
end, insert the needle back through into the lumen and introduce a
continuous, unlocked, spiral stitch joining the back walls as far as
the other end.
• If the line of anastomosis lies in the sagittal plane, start at the near
end, complete the stitching of the back wall, continue round the
far corner and close the anterior walls from far to near, to reach the
starting point.
• For a right-handed surgeon, to avoid this, at the far end, having
passed the needle through to the left side, reverse the needle and
pass it from within out, creating a loop on the mucosa – a single
‘Connell’ stitch. You can now continue to sew naturally, driving the
needle from right to left along the anterior wall, to reach the
starting point. Remove and discard the needle and tie the free end
to the clamped short end.
23.
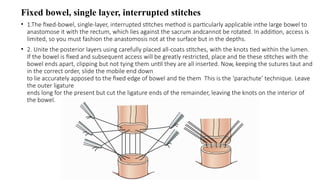
Fixed bowel, singlelayer, interrupted stitches
• 1.The fixed-bowel, single-layer, interrupted stitches method is particularly applicable inthe large bowel to
anastomose it with the rectum, which lies against the sacrum andcannot be rotated. In addition, access is
limited, so you must fashion the anastomosis not at the surface but in the depths.
• 2. Unite the posterior layers using carefully placed all-coats stitches, with the knots tied within the lumen.
If the bowel is fixed and subsequent access will be greatly restricted, place and tie these stitches with the
bowel ends apart, clipping but not tying them until they are all inserted. Now, keeping the sutures taut and
in the correct order, slide the mobile end down
to lie accurately apposed to the fixed edge of bowel and tie them This is the ‘parachute’ technique. Leave
the outer ligature
ends long for the present but cut the ligature ends of the remainder, leaving the knots on the interior of
the bowel.
24.
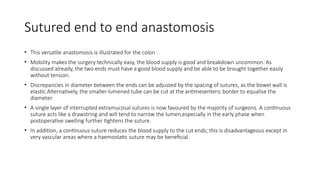
Sutured end toend anastomosis
• This versatile anastomosis is illustrated for the colon .
• Mobility makes the surgery technically easy, the blood supply is good and breakdown uncommon. As
discussed already, the two ends must have a good blood supply and be able to be brought together easily
without tension.
• Discrepancies in diameter between the ends can be adjusted by the spacing of sutures, as the bowel wall is
elastic.Alternatively, the smaller-lumened tube can be cut at the antimesenteric border to equalise the
diameter.
• A single layer of interrupted extramucosal sutures is now favoured by the majority of surgeons. A continuous
suture acts like a drawstring and will tend to narrow the lumen,especially in the early phase when
postoperative swelling further tightens the suture.
• In addition, a continuous suture reduces the blood supply to the cut ends; this is disadvantageous except in
very vascular areas where a haemostatic suture may be beneficial.
25.
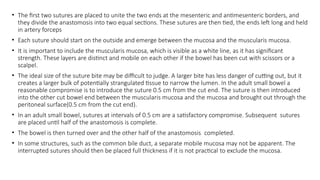
• The firsttwo sutures are placed to unite the two ends at the mesenteric and antimesenteric borders, and
they divide the anastomosis into two equal sections. These sutures are then tied, the ends left long and held
in artery forceps
• Each suture should start on the outside and emerge between the mucosa and the muscularis mucosa.
• It is important to include the muscularis mucosa, which is visible as a white line, as it has significant
strength. These layers are distinct and mobile on each other if the bowel has been cut with scissors or a
scalpel.
• The ideal size of the suture bite may be difficult to judge. A larger bite has less danger of cutting out, but it
creates a larger bulk of potentially strangulated tissue to narrow the lumen. In the adult small bowel a
reasonable compromise is to introduce the suture 0.5 cm from the cut end. The suture is then introduced
into the other cut bowel end between the muscularis mucosa and the mucosa and brought out through the
peritoneal surface(0.5 cm from the cut end).
• In an adult small bowel, sutures at intervals of 0.5 cm are a satisfactory compromise. Subsequent sutures
are placed until half of the anastomosis is complete.
• The bowel is then turned over and the other half of the anastomosis completed.
• In some structures, such as the common bile duct, a separate mobile mucosa may not be apparent. The
interrupted sutures should then be placed full thickness if it is not practical to exclude the mucosa.
27.
Sutured end toside anastomosis
• An end-to-side sutured anastomosis is merely an adaptation of the end-to-end technique.
• An incision is made in the side of the viscus to which the end is to be joined. The length of the incision should
be such that there are two equal ‘lumens’ for the anastomosis. The suture technique used is similar to that
described for an end-to-end anastomosis.
28.
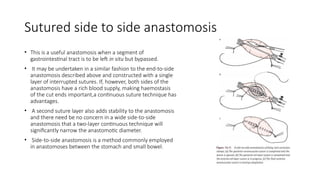
Sutured side toside anastomosis
• This is a useful anastomosis when a segment of
gastrointestinal tract is to be left in situ but bypassed.
• It may be undertaken in a similar fashion to the end-to-side
anastomosis described above and constructed with a single
layer of interrupted sutures. If, however, both sides of the
anastomosis have a rich blood supply, making haemostasis
of the cut ends important,a continuous suture technique has
advantages.
• A second suture layer also adds stability to the anastomosis
and there need be no concern in a wide side-to-side
anastomosis that a two-layer continuous technique will
significantly narrow the anastomotic diameter.
• Side-to-side anastomosis is a method commonly employed
in anastomoses between the stomach and small bowel.
29.
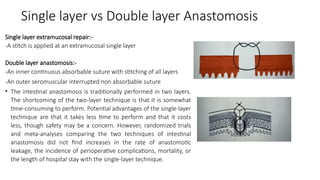
Single layer vsDouble layer Anastomosis
Single layer extramucosal repair:-
-A stitch is applied at an extramucosal single layer
Double layer anastomosis:-
-An inner continuous absorbable suture with stitching of all layers
-An outer seromuscular interrupted non absorbable suture
• The intestinal anastomosis is traditionally performed in two layers.
The shortcoming of the two-layer technique is that it is somewhat
time-consuming to perform. Potential advantages of the single-layer
technique are that it takes less time to perform and that it costs
less, though safety may be a concern. However, randomized trials
and meta-analyses comparing the two techniques of intestinal
anastomosis did not find increases in the rate of anastomotic
leakage, the incidence of perioperative complications, mortality, or
the length of hospital stay with the single-layer technique.
31.
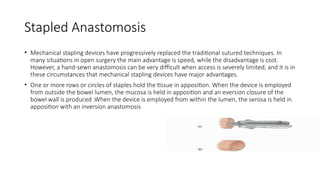
Stapled Anastomosis
• Mechanicalstapling devices have progressively replaced the traditional sutured techniques. In
many situations in open surgery the main advantage is speed, while the disadvantage is cost.
However, a hand-sewn anastomosis can be very difficult when access is severely limited, and it is in
these circumstances that mechanical stapling devices have major advantages.
• One or more rows or circles of staples hold the tissue in apposition. When the device is employed
from outside the bowel lumen, the mucosa is held in apposition and an eversion closure of the
bowel wall is produced .When the device is employed from within the lumen, the serosa is held in
apposition with an inversion anastomosis
32.
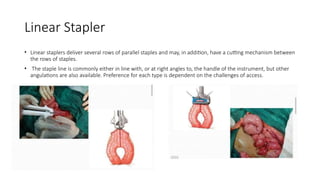
Linear Stapler
• Linearstaplers deliver several rows of parallel staples and may, in addition, have a cutting mechanism between
the rows of staples.
• The staple line is commonly either in line with, or at right angles to, the handle of the instrument, but other
angulations are also available. Preference for each type is dependent on the challenges of access.
33.
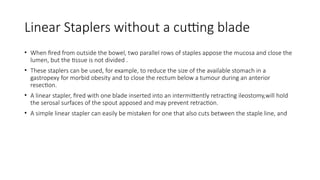
Linear Staplers withouta cutting blade
• When fired from outside the bowel, two parallel rows of staples appose the mucosa and close the
lumen, but the tissue is not divided .
• These staplers can be used, for example, to reduce the size of the available stomach in a
gastropexy for morbid obesity and to close the rectum below a tumour during an anterior
resection.
• A linear stapler, fired with one blade inserted into an intermittently retracting ileostomy,will hold
the serosal surfaces of the spout apposed and may prevent retraction.
• A simple linear stapler can easily be mistaken for one that also cuts between the staple line, and
34.
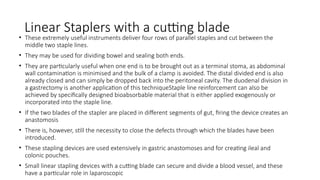
Linear Staplers witha cutting blade
• These extremely useful instruments deliver four rows of parallel staples and cut between the
middle two staple lines.
• They may be used for dividing bowel and sealing both ends.
• They are particularly useful when one end is to be brought out as a terminal stoma, as abdominal
wall contamination is minimised and the bulk of a clamp is avoided. The distal divided end is also
already closed and can simply be dropped back into the peritoneal cavity. The duodenal division in
a gastrectomy is another application of this techniqueStaple line reinforcement can also be
achieved by specifically designed bioabsorbable material that is either applied exogenously or
incorporated into the staple line.
• If the two blades of the stapler are placed in different segments of gut, firing the device creates an
anastomosis
• There is, however, still the necessity to close the defects through which the blades have been
introduced.
• These stapling devices are used extensively in gastric anastomoses and for creating ileal and
colonic pouches.
• Small linear stapling devices with a cutting blade can secure and divide a blood vessel, and these
have a particular role in laparoscopic
35.
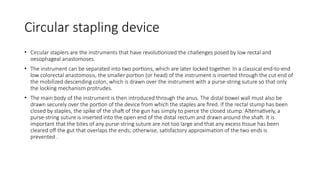
Circular stapling device
•Circular staplers are the instruments that have revolutionized the challenges posed by low rectal and
oesophageal anastomoses.
• The instrument can be separated into two portions, which are later locked together. In a classical end-to-end
low colorectal anastomosis, the smaller portion (or head) of the instrument is inserted through the cut end of
the mobilized descending colon, which is drawn over the instrument with a purse-string suture so that only
the locking mechanism protrudes.
• The main body of the instrument is then introduced through the anus. The distal bowel wall must also be
drawn securely over the portion of the device from which the staples are fired. If the rectal stump has been
closed by staples, the spike of the shaft of the gun has simply to pierce the closed stump. Alternatively, a
purse-string suture is inserted into the open end of the distal rectum and drawn around the shaft. It is
important that the bites of any purse-string suture are not too large and that any excess tissue has been
cleared off the gut that overlaps the ends; otherwise, satisfactory approximation of the two ends is
prevented .
36.
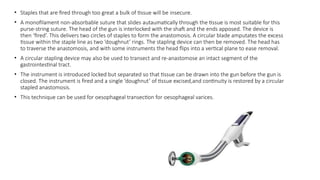
• Staples thatare fired through too great a bulk of tissue will be insecure.
• A monofilament non-absorbable suture that slides autaumatically through the tissue is most suitable for this
purse-string suture. The head of the gun is interlocked with the shaft and the ends apposed. The device is
then ‘fired’. This delivers two circles of staples to form the anastomosis. A circular blade amputates the excess
tissue within the staple line as two ‘doughnut’ rings. The stapling device can then be removed. The head has
to traverse the anastomosis, and with some instruments the head flips into a vertical plane to ease removal.
• A circular stapling device may also be used to transect and re-anastomose an intact segment of the
gastrointestinal tract.
• The instrument is introduced locked but separated so that tissue can be drawn into the gun before the gun is
closed. The instrument is fired and a single ‘doughnut’ of tissue excised,and continuity is restored by a circular
stapled anastomosis.
• This technique can be used for oesophageal transection for oesophageal varices.
37.
Types of Intestinalstaplers used
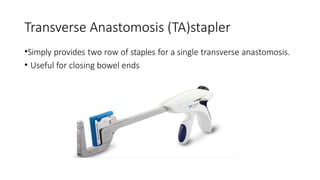
•Transverse anastomosis (TA) stapler
•Gastrointestinal anastomosis (GIA) stapler
•Circular or end-to-end anastomosis(EEA)stapler
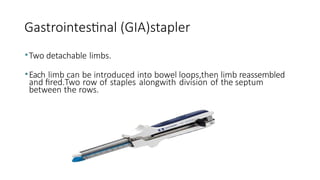
Gastrointestinal (GIA)stapler
•Two detachablelimbs.
•Each limb can be introduced into bowel loops,then limb reassembled
and fired.Two row of staples alongwith division of the septum
between the rows.
43.
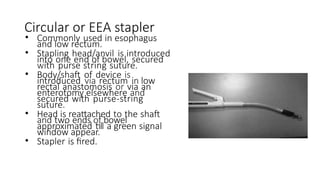
Circular or EEAstapler
• Commonly used in esophagus
and low rectum.
• Stapling head/anvil is introduced
into one end of bowel, secured
with purse string suture.
• Body/shaft of device is
introduced via rectum in low
rectal anastomosis or via an
enterotomy elsewhere and
secured with purse-string
suture.
• Head is reattached to the shaft
and two ends of bowel
approximated till a green signal
window appear.
• Stapler is fired.
46.
Complications
• Anastomotic leakage
•Wound Fistuae
• Bleeding
• Wound infection
• Anastomotic stricture
• Prolonged functional ileus, especially in children
• Rarely,Anastomotic ulcers of jejunum in cases of gastrojejunostomy.
47.
Anastomotic Leakage
• Anastomoticleakage is the most feared early complication of intestinal
anastomosis. The healing of an intestinal anastomosis is broadly
divided into three phases, as follows:
1. Inflammatory phase
2. Fibroplasia phase
3. Remodeling phase
48.
• During theinflammatory phase, the integrity of the anastomosis is
dependent on mechanical strength provided by sutures.
• The inflammatory phase is followed by the fibroplasia phase around
postoperative days 5-7; this phase is characterized by a switch from
collagen degradation to collagen deposition, which gives strength to
the anastomosis.
• Any systemic or local factor that causes delay in the transition from
the inflammatory phase to the fibroplasia phase can result in poor
healing and anastomotic leakage.
49.
Sequence of anastomoticleak
• Post operative day (POD)3: Fever more than 38 degree Celsius
• POD 2-4 : Amount of drainage fluid increasing most likely due to technical
errors, as the bowel has oedema, where if we give loose stitch. It can cut
through. After 48 hrs as soon as peristalsis return , leak occurs
• POD 4- Absence of bowel movements, amount of drainage fluid increasing
• POD 6 – Increase in total leukocyte count
• Mean post operative period for anastomotic leak – POD 5 to 16 mostly
due to increased pressure, ischaemic necrosis of anastomosis
50.
• Systemic conditionsthat increase the risk of anastomotic leakage are anemia, diabetes mellitus,
malnutrition with hypoalbuminemia, vitamin deficiencies, and steroid therapy. Local factors such as
the presence of irradiated bowel, anastomosis involving disease-affected bowel, and inadequate
blood flow are associated with poor healing and anastomotic leakage.
• Anastomotic leakage presenting on postoperative day 1 or 2 is invariably due to technical reasons.
Anastomotic leakage secondary to interference in the normal healing mechanism usually presents
around the end of postoperative week 1. Anastomotic leakage can present either as frank peritonitis
when the leak is uncontrolled or as localized intra-abdominal collection/abscess if the leak is
controlled.
• An uncontrolled leak with diffuse peritonitis is associated with high morbidity and mortality and
necessitates re-exploration. During repeat laparotomy, a thorough lavage of the peritoneal cavity
should be carried out. In most circumstances, it is better to dismantle the anastomosis and bring out
the bowel loops as a stoma. A controlled leak presenting with a localized intra-abdominal abscess can
be managed conservatively with percutaneous drainage of the abscess under imaging guidance and
antibiotics.
• The management of leaks depends on whether they are early or late, whether they are from large or
small bowel and whether there is generalised peritoneal soiling, a localized collection or fistulation.
51.
Management
Suspicion of anyleak should be managed first conservatively
• Immediate resuscitation.
• Correction for third space loss and Intestinal content losses.
• Npo, if orally started.
• Infected surgical wo und should be drained.
• Blood transfusion if required.
• Broad spectrum antibiotics.
Reoperation is indicated in the following:-
• Diffuse peritonitis.
• Intraabdominal haemorrhage.
• Suspected intestinal ischaemia.
52.
Generalised Peritonitis
• Ananastomotic leak that presents as a generalised peritonitis will require reoperation. The peritoneal cavity is
cleared of small bowel contents or faeculent material. A simple repair of a defect is seldom practical as the
tissues are friable and oedematous.
• Gastric and duodenal anastomotic leaks may sometimes be managed by oversewing of the defect and
diversional bypass.
• Other solutions include a more radical resection and reanastomosis or the use of a Roux loop brought up as
the drainage conduit of an internal fistula. In an ileal or ileocolic anastomosis the safest management is to
bring out an ileostomy with the proximal end. The distal end can be closed or brought out as a mucous fistula
adjacent to the ileostomy. The latter is safer and also makes the subsequent operation to restore intestinal
continuity simpler.
• A leaking jejunal anastomosis is not so suitable for this management as the stoma will have a very high output.
The situation may be better managed by resection and reanastomosis.
• In colonic leaks, if the anastomosis is above the peritoneal reflection, the safest manoeuvre may be to detach
the anastomosis fully and bring out the proximal end as an end stoma.
• The distal end is safest if brought out as a mucous fistula, and if this is adjacent to the proximal stoma,
subsequent surgery to restore gastrointestinal continuity is less complex.
53.
Pelvic Peritonitis
• Pelvicperitonitis after a leak from the anastomosis following an anterior resection requires intervention, even if the
peritonitis is initially confined to the pelvis. Treatment by taking down the anastomosis and forming an end stoma
will almost certainly condemn the patient to a permanent colostomy, as any rejoin at a very low level is difficult and
function is almost invariably poor. A better alternative is to select an area of the transverse colon that is suitable for
a loop colostomy.
Sealed Leak
• A leak may seal and present as a localised intraperitoneal collection with an associated ileus or small bowel
obstruction.
• Conservative management with intravenous fluids and antibiotics will often suffice, but drainage of the collection
may become necessary. A localised collection of infected gastrointestinal contents, walled off within the peritoneal
cavity, may track into another viscus or to the exterior via the vagina or the surgical wound. When there is still a
leak from the anastomosis into the walled-off collection, a fistula will have beenestablished.
54.
Wound Fistulae
• Awound fistula usually presents initially as a simple wound infection. It then becomes apparent
that intestinal contents are draining through the wound. Immediate repair is not advisable and the
initial management is maintenance of fluid and electrolyte balance, drainage of infection,
maintenancenof nutrition and protection of the abdominal skin from intestinal juices.
• Ultrasound scans will show whether there is an intra-abdominal collection deep to the wound and,
if there is, drainage of this should be improved.
• If defaecation or a more distal stoma effluent continues, there is still continuity of the
gastrointestinal tract and the fistula track may close spontaneously if there is no distal obstruction.
When the fistula is from the duodenum or jejunum, parenteral feeding is preferable initially if
spontaneous resolution seems probable, as this will reduce fistula losses and healing is more likely.
• There is little advantage in restricting oral intake in cases of colonic faecal fistulae.
55.
• A persistentfistula will require surgical repair. The dissection of a small bowel fistula and the anastomosis will
be relatively straightforward if the fistula has been allowed to mature.
• A mature small bowel fistula starts to prolapse, similar to an ileostomy spout, as the peritoneal cavity reforms.
• This will usually require a delay of around 6–12 months, during which time it is important that nutrition is
maintained.
• Unless the fistula is of very high output, enteral feeding is preferable to intravenous feeding during this period.
The‘neo-stoma’ of a faecal colonic fistula should also be allowed to mature before further surgery is
undertaken to restore intestinal continuity
56.
Bleeding
• Bleeding-related complicationsafter intestinal anastomosis are common in patients with sepsis and
deranged coagulopathy. Bleeding may manifest in the immediate postoperative period as
hemorrhagic aspirate from the nasogastric tube, hematemesis, melena, or bleeding from an intra-
abdominal drain.
• Patients with bleeding should be aggressively managed with correction of coagulopathy (if present)
and blood transfusion. If the bleeding results in hemodynamic instability with a significant decrease
in hemoglobin, urgent reexploration should be performed. Intraoperative anastomotic site bleeding
is characterized by blood in the intestinal lumen distal to the anastomosis. In such circumstances, the
anterior layer of the sutures is opened and both layers are examined for evidence of any bleeding.
• Once the bleeding site is identified, it can be controlled with hemostatic sutures. The decision to
reanastomose or to convert into a stoma depends on the general condition of the patient.
Conversion to a stoma is preferred in patients who are hemodynamically unstable.
57.
Wound Infection
• Woundinfection occurs when there is uncontrolled spillage of
intestinal contents during anastomosis.
• It is managed by removing a few skin sutures and ensuring proper
drainage of pus.
• Superficial surgical-site infection does not require treatment with
systemic antibiotics.
58.
Anastomotic stricture
• Anastomoticstricture is a late complication of intestinal anastomosis.
• The risk of anastomotic stricture is marginally increased after end-to-end
anastomosis, especially when the anastomosis is performed with a stapled
technique.
• The most important risk factor for anastomotic stricture is a controlled
anastomotic leak managed conservatively. This scenario is more common after
cervical esophageal and colorectal anastomotic leaks. Anastomotic strictures
occurring in these areas can be conservatively managed with endoscopic or
colonoscopic dilatation. If this fails, surgical revision might be required


![• The next step is division of the bowel. This is done by applying a noncrushing clamp on the bowel
end used for anastomosis and applying crushing clamps on the bowel to be resected so that the
intraluminal contents of the resected bowel do not contaminate the peritoneal cavity. Clamps are
applied from the antimesenteric end, and care should be taken to avoid crushing of the
mesentery.
• The bowel is divided with a knife close to the crushing clamp so as to preserve adequate bowel
length distal to a noncrushing clamp for anastomosis. The direction of division is oblique to ensure
an adequate lumen and to maintain a longer length of the mesenteric end as compared with the
antimesenteric end. The specimen is removed with clamps in situ.
• While dividing the bowel , we should divide the bowel well in advance, then wash peritoneal
cavity for minimum 20 minutes then we should go for anastomosis
• Care should be taken to avoid spillage of enteric contents during bowel division. Alternatively,
bowel division can also done with a linear cutting (gastrointestinal anastomosis [GIA]) stapler,
which divides and seals two cut ends simultaneously, thereby preventing fecal contamination as
fecal contamination is a negative factor for intestinal anastomosis](https://image.slidesharecdn.com/resectionandanastomosis-250403182703-83da92d3/85/Resection-and-Anastomosis-pptx-pptx-pptx-16-320.jpg)