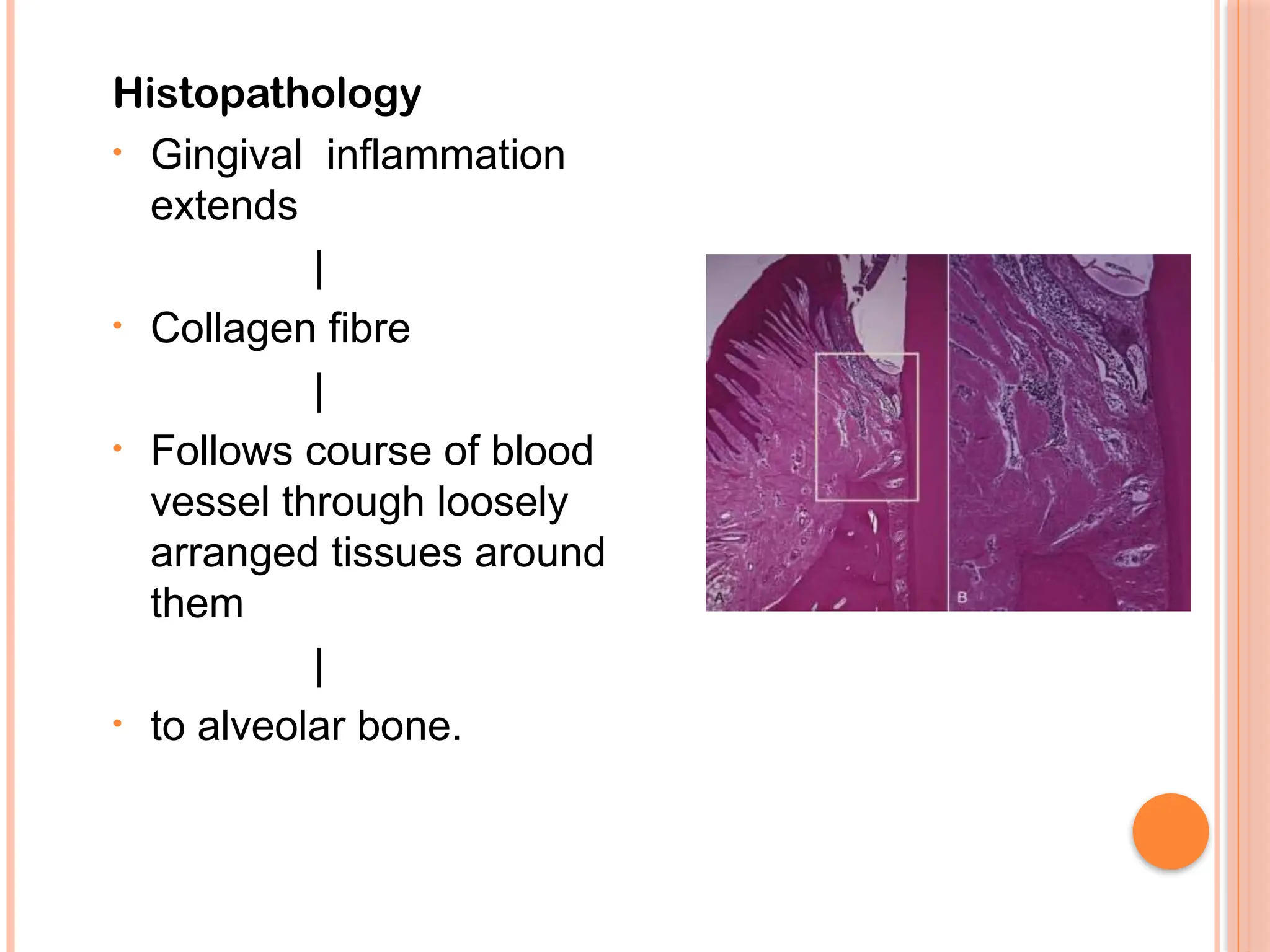
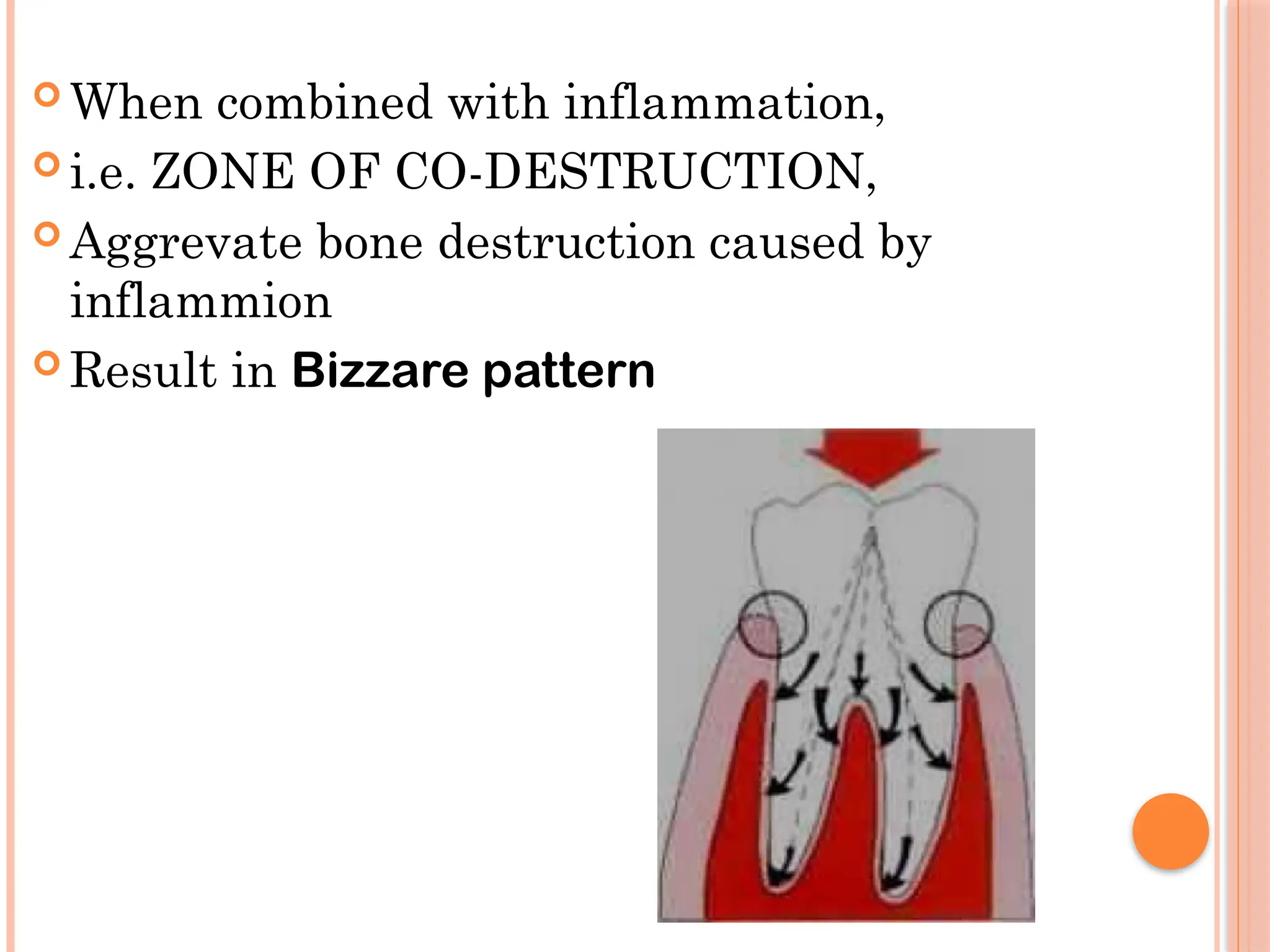
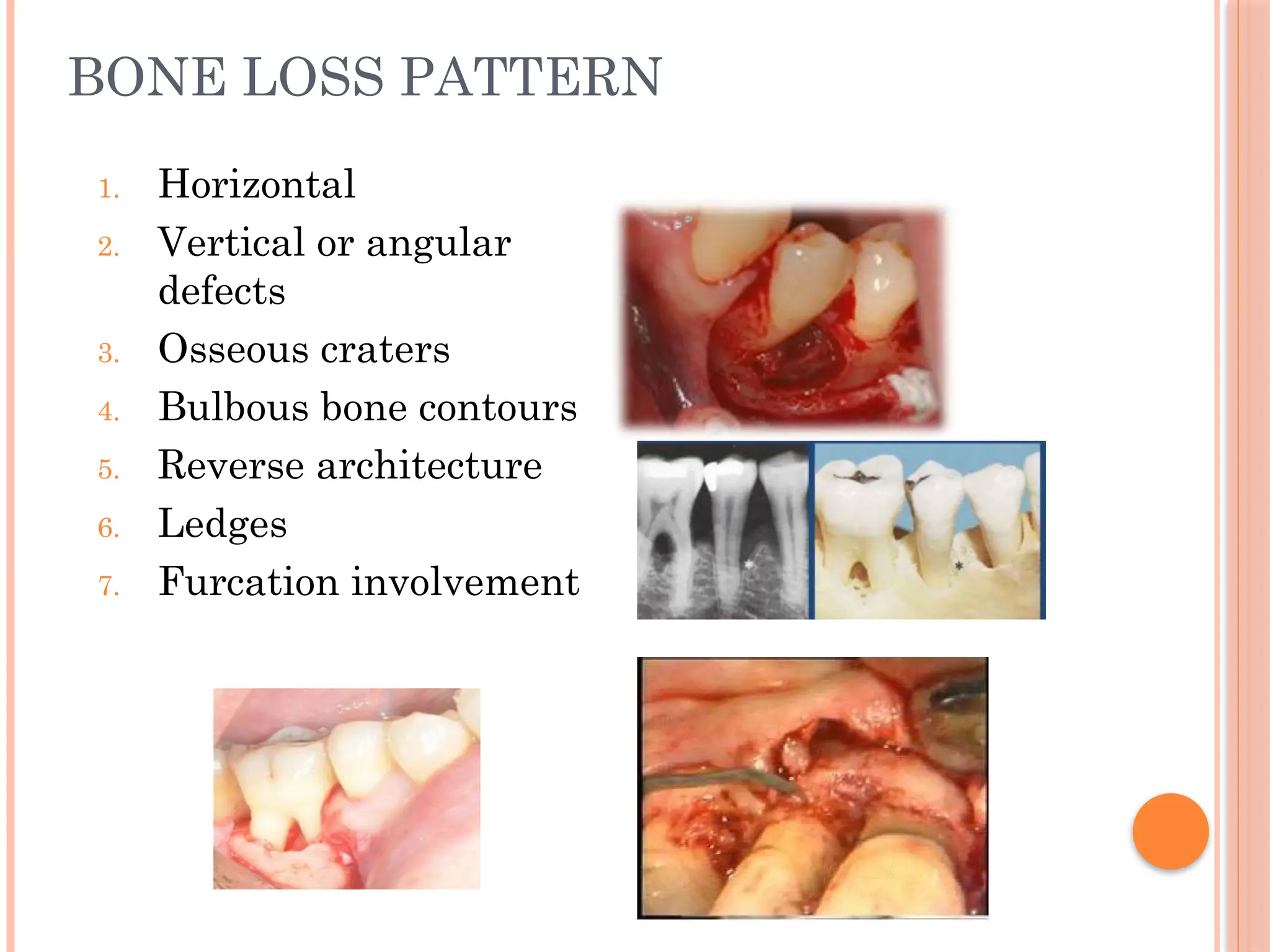
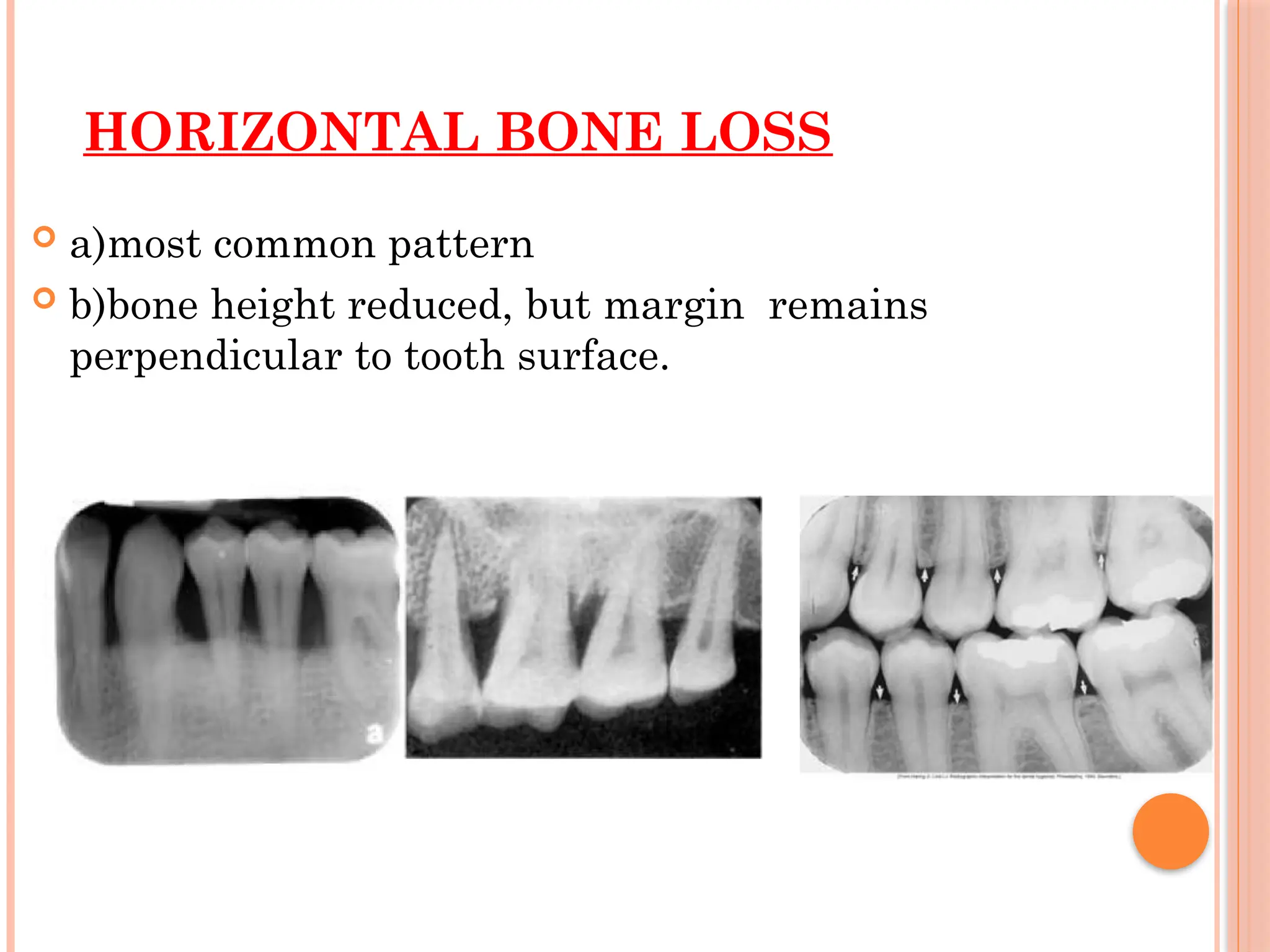
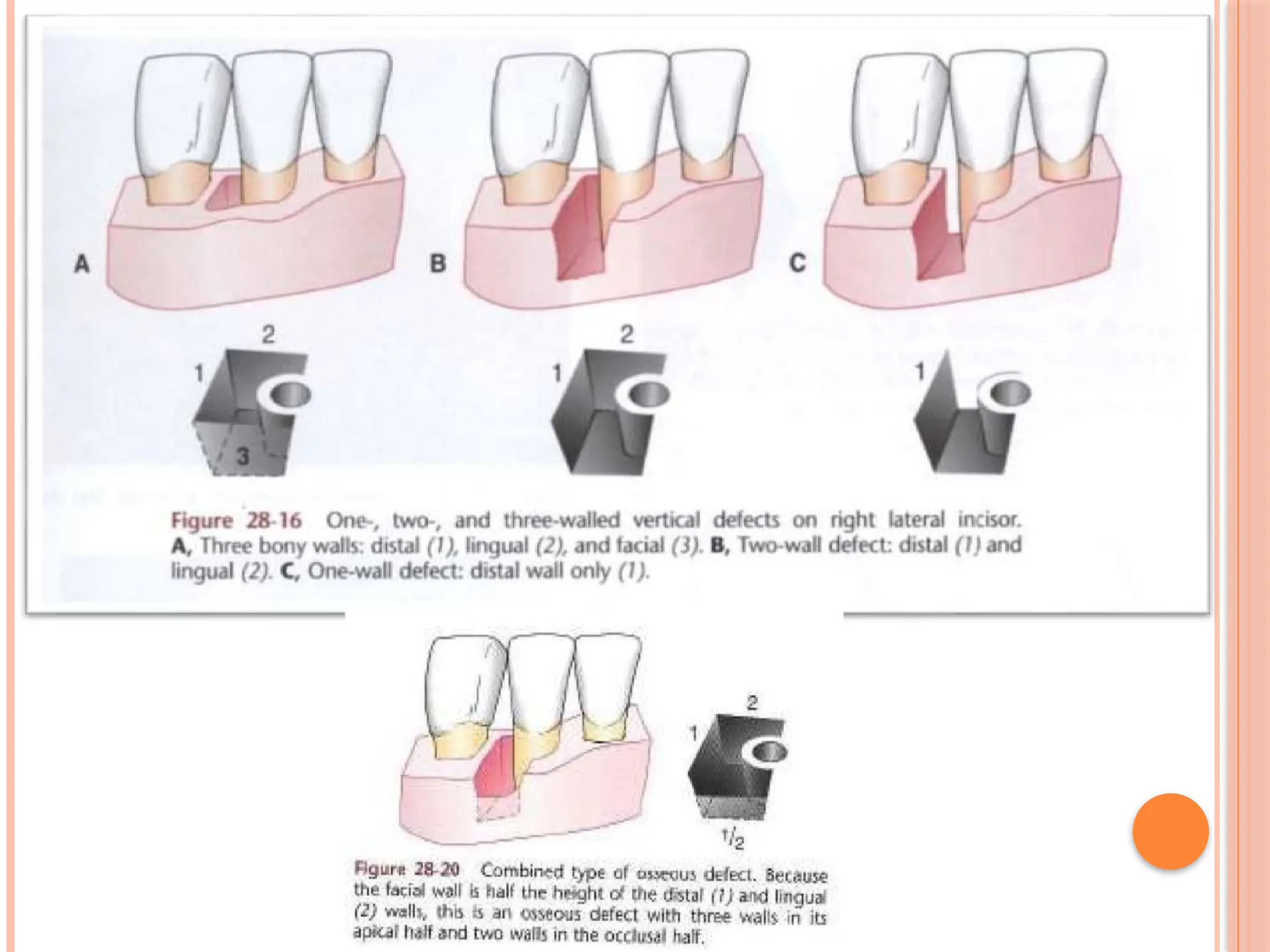
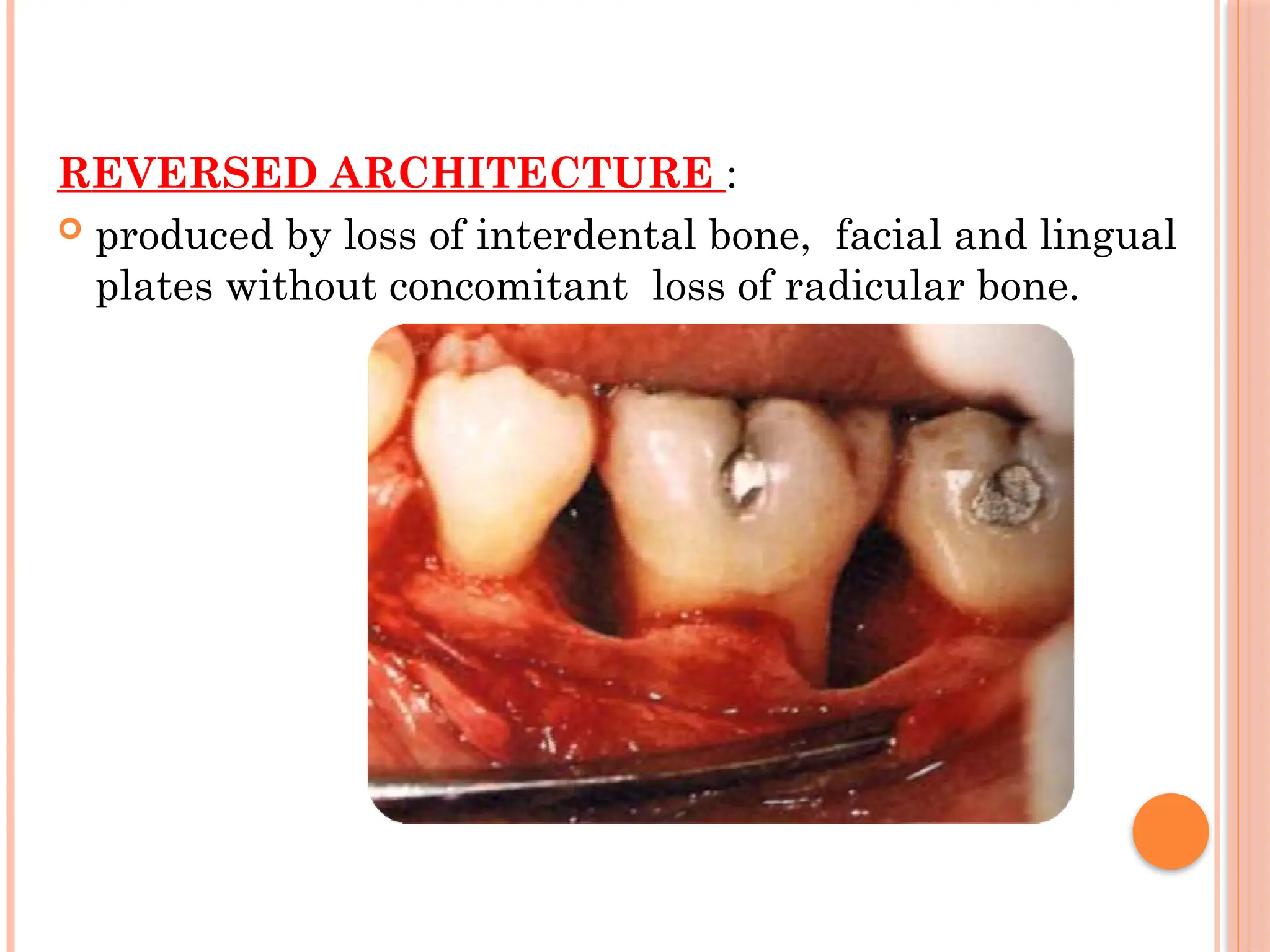
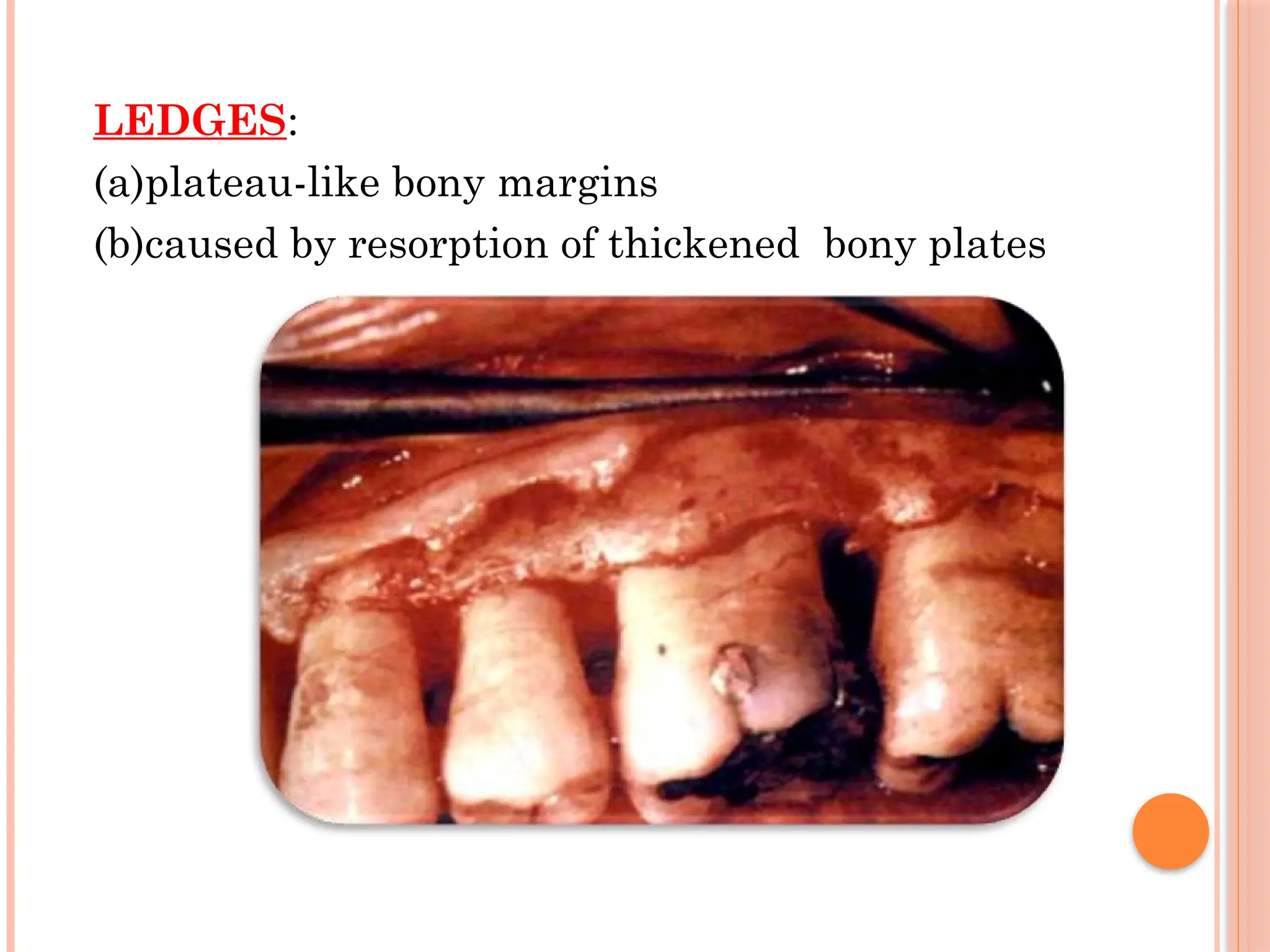
The document discusses bone loss and patterns of bone destruction in the context of periodontitis, emphasizing that bone destruction leads to tooth loss and is influenced by various factors including inflammation, trauma, and systemic disorders. It details the histopathology of bone loss, different types of bone defects, and classifications of furcation involvement, providing insight into how periodontal disease affects bone morphology. Various patterns of bone destruction, such as horizontal and vertical bone loss, are also described, outlining their implications for periodontal health.