Downloaded 13 times








![1.Nephroptosis (Asymptomatic)
Downward displacement of kidney by more than two
vertebral bodies or 5 cm
40 patients (24.3%)
[bilateral (n=15), unilateral (n=25)]
Results](https://image.slidesharecdn.com/bno-ivperect-160711021813/85/Bno-ivp-erect-12-320.jpg)

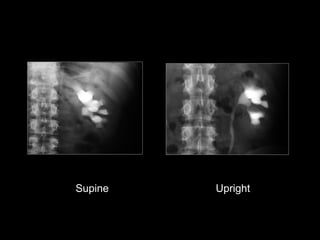
![2. Better filling of collecting system
9 patients (5.4%)
[ureteral filling (n= 8),
upper pole infindibular filling (n=1) ]
Results](https://image.slidesharecdn.com/bno-ivperect-160711021813/85/Bno-ivp-erect-15-320.jpg)









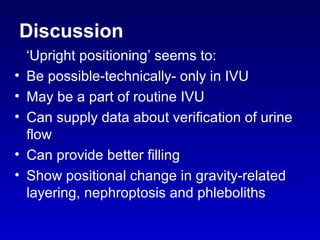

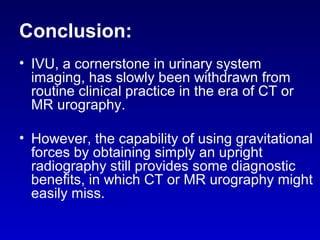

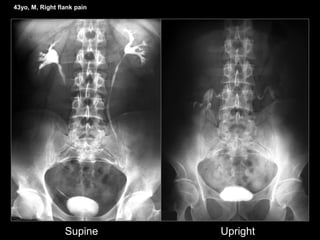
This study assessed the diagnostic value of obtaining an additional upright kidney-ureter-bladder (KUB) radiograph during routine intravenous urography (IVU). Of 164 patients who underwent IVU with an additional upright KUB, the upright view provided diagnostic benefit in 72 patients (43.9%), identifying issues like nephroptosis, better filling of the collecting system, differentiation of phleboliths from stones, and evaluation of emptying. While newer modalities have advantages, upright positioning remains a simple way for IVU to provide unique diagnostic information by leveraging gravitational effects.









































































