















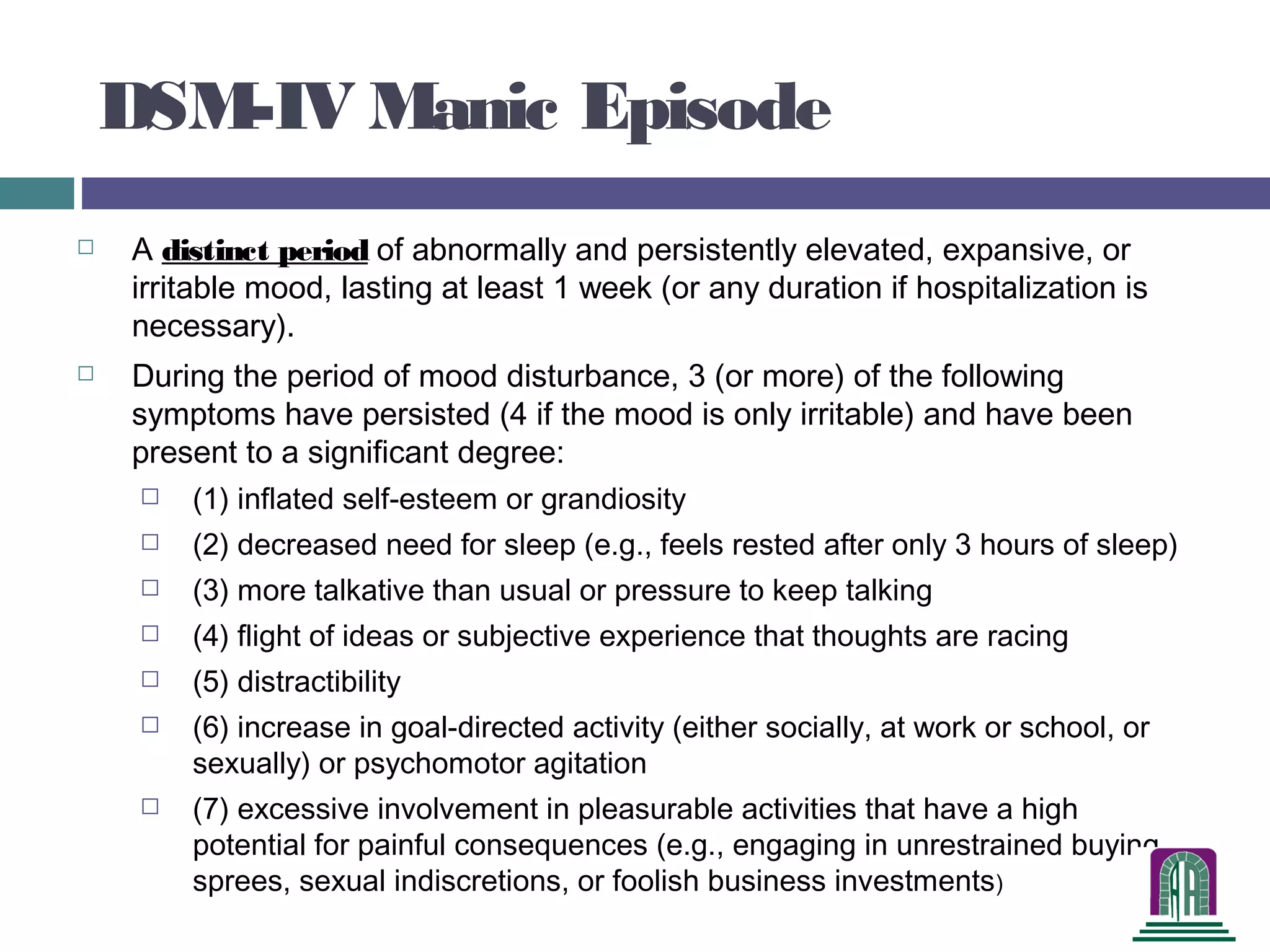












































The document provides a comprehensive overview of bipolar disorder in children and adolescents, focusing on diagnosis and treatment options for educational professionals. It discusses the historical context of New Jersey's mental health services reform and outlines significant changes in care, emphasizing family and community-based approaches. The text also details diagnostic criteria, treatment modalities, and the challenges in accurately diagnosing and managing pediatric bipolar disorder.