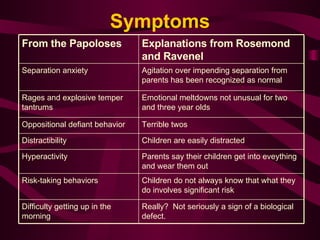
The document discusses the controversy around diagnosing pediatric bipolar disorder. It outlines key perspectives, diagnostic criteria, and a lack of conclusive research evidence. Symptoms used to diagnose bipolar disorder in children are subjective and overlap with other disorders. International views show more skepticism about the validity of the diagnosis in pre-pubescent children. Further research is still needed to definitively diagnose or rule out the existence of bipolar disorder in young children.
![In its practice guidelines for pediatricians, states: “ DSM-IV criteria remain a consensus without clear empirical [research] data supporting the number of items required for the diagnosis. . . Furthermore, the behavioral characteristics specified in DSM-IV, despite efforts to standardize them, remain subjective.” American Academy of Pediatrics](https://image.slidesharecdn.com/kellypediatricbipolar-090513130732-phpapp02/85/Kelly-Pediatric-Bipolar-8-320.jpg)