Download to read offline













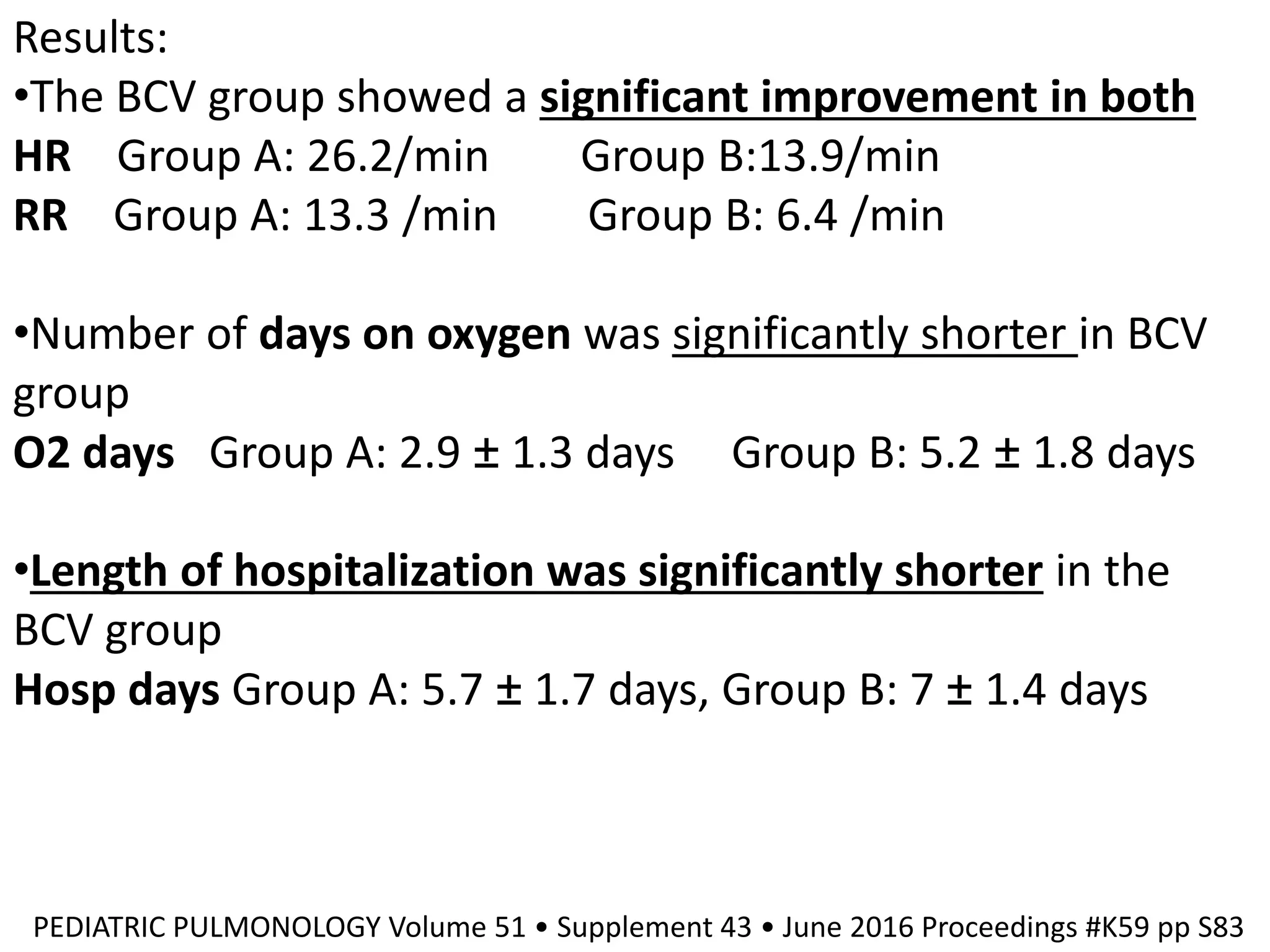



























































The document discusses biphasic cuirass ventilation (BCV) as a treatment for various forms of respiratory failure, emphasizing its benefits such as improved gas exchange, decreased work of breathing, and reduced hospitalization rates. Studies also reveal the efficacy of combining positive and negative ventilation strategies, particularly in patients with acute respiratory distress syndrome (ARDS) and chronic obstructive pulmonary disease (COPD). Overall, BCV and related strategies show promise in enhancing patient outcomes by preventing intubations and decreasing medical costs.



































































