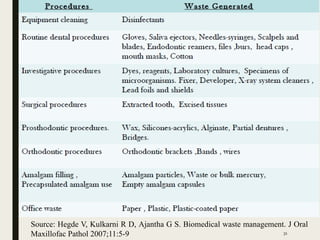
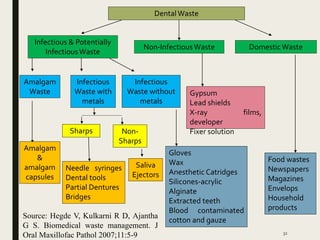
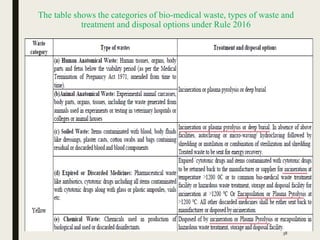
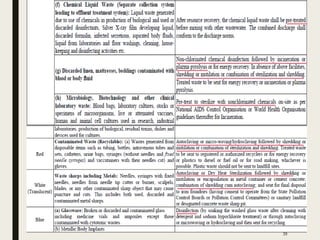
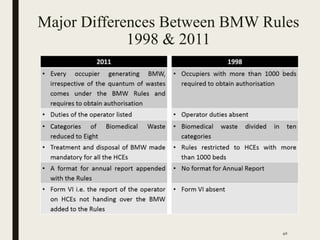
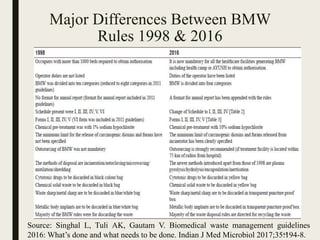
This document provides an overview of healthcare waste management presented by Dr. Radhika Mitra. It begins with an introduction to the increasing amounts of waste generated by hospitals and the health risks posed by improper management. The presentation then covers classifications of healthcare waste, sources, composition, hazards, and regulations in India. Specific sections discuss the categories of waste generated in dental settings, treatment and disposal techniques, and the steps needed for proper waste management in dental camps or clinics.